


Featured Articles
What separates high- and low-performing hospitals in 2025

Hospital finances showed signs of improvement at the end of the second quarter, though notable performance gaps remain between higher- and lower-performing facilities, according to Kaufman Hall’s latest “National Hospital Flash Report,” published Aug. 11.
The median monthly operating margin index rose to 3.7% in June, up from 1.9% in May, though the pace of improvement remains uneven and somewhat unexpected amid recent market turbulence.
Hospitals in the Northeast and Mid-Atlantic reported the largest year-over-year increases in operating margins at 38%, followed by the South and Midwest at 29%. The West and Great Plains saw declines of 13% and 27%, respectively. Smaller and mid-size hospitals generally fared better than large facilities: hospitals with 26 to 299 beds saw margin gains between 17% and 30%, while those with more than 500 beds experienced a 29% decline.
“Higher performing hospitals are nimbler on both the revenue and expense sides,” Erik Swanson, managing director and data and analytics group leader at Kaufman Hall, said in a news release. “They may be expanding their outpatient footprint, diversifying services or managing expenses like purchased services by centralizing some functions. They are also more likely to have value-based care or bundled care arrangements in place.”
In 2025, top-performing hospitals are setting themselves apart from lower-performing facilities through a combination of strategic, operational and financial factors. According to Kaufman Hall and Fitch Ratings, the key differentiators include:
1. Strong market presence in growth regions: Hospitals located in expanding markets — especially in the South, Midwest and Northeast — are benefiting from rising demand, better payer mixes and stronger revenue potential. These organizations are leveraging local demographics and economic growth to drive performance.
2. Workforce recruitment and retention. Talent remains a key differentiator. High performers are more successful in hiring and retaining clinical and nonclinical staff amid national shortages, allowing them to maintain service capacity and quality care while controlling labor costs.
3. Aggressive payer strategy: Top-tier hospitals are skilled at negotiating favorable payer contracts, often using a “mind the gap” approach to keep reimbursement rates at the upper end of the scale. These hospitals maximize market leverage to drive revenue growth.
4. Operational agility: High-performing hospitals are nimble and can adjust quickly to changing conditions. They centralize purchased services, optimize supply chains and adapt care models to improve efficiency.
5. Investment in technology and infrastructure: Successful systems are proactively investing in AI, health IT and data analytics. These investments support care delivery and administrative efficiency and prepare hospitals for value-based care and alternative payment models.
6. Outpatient expansion and service diversification: Expanding outpatient footprints and diversifying service lines allow top hospitals to meet evolving patient demand and offset pressures on inpatient care, particularly in high-cost settings.
7. Proactive real estate and capital management. Strong performers are strategically managing real estate assets to bolster balance sheets and fund growth initiatives, such as facility modernization and digital transformation.
In contrast, lower-performing hospitals, often in rural or underserved regions, struggle with:
- Limited access to capital
- Declining patient volumes or poor payer mixes
- Severe staffing shortages
- High dependency on public reimbursement
- Little room for investment in innovation or infrastructure
Fitch warns that this divergence is becoming a “trifurcation” of hospital performance, with institutions separating into top-tier, middle-tier and lower-tier segments. Without strategic shifts, the financial gap may widen in the years ahead.
Top-performing hospitals will “have a predisposition to maximize that market essentially with annual payer negotiations, in a ‘mind the gap’ mentality that keeps them at the upper end of the payment scale,” Fitch said in a recent report.
Meanwhile, most hospitals are expected to remain in a middle band: operating sustainably but with limited margin growth and persistent staffing challenges. Those at the bottom of the scale face declining volume and payer mix issues and will likely need to rely heavily on outside cash to stabilize, according to Fitch.
The latest hospital financial reports indicate that 2025 performance gains are unevenly distributed, with the gap between top and bottom performers potentially widening as financial pressures persist.

How to Get a High Paying Contract Nursing Job
Contract nursing offers the chance to do meaningful work, gain diverse experience, and earn competitive pay. Whether you’re pursuing contract nursing jobs, per diem nursing positions, or rapid response assignments, the key to maximizing your income is preparation and strategy.
If you’re ready to secure a high-paying contract nursing job, use these proven tips to set yourself apart and negotiate pay that reflects your expertise.
Your resume is your first impression. A clear, polished resume highlights your skills, certifications, and professional accomplishments, and it determines whether you’ll be invited to interview.
Include:
- Your nursing specialties (such as ICU, emergency department, or medical imaging)
- Certifications (like ACLS, BLS, or specialty credentials)
- Details about your experience in different care settings, such as inpatient care, skilled nursing facilities, or acute care staffing
It’s normal to have employment gaps but be ready to confidently explain them during interviews. A well-organized resume positions you as a serious professional ready for high-paying nursing contracts.
Keeping your credentials updated makes you a more attractive candidate and can improve your earning potential.
Make sure to:
- Renew essential licenses and certifications promptly.
- Consider adding specialty certifications that are in demand for travel nursing jobs and contract assignments.
- Stay up to date with immunizations required by hospitals and clinics. Being ready with all documentation can speed up onboarding and help you access crisis response nursing jobs or urgent needs contracts that often pay premium rates.
The more prepared you are, the easier it is for a nurse staffing agency or recruiter to match you with higher-paying positions.
Professional references can be the deciding factor in landing a top-paying assignment.
Employers and recruiters rely on references to verify your:
- Clinical skills
- Professionalism
- Reliability
Choose references who can confidently speak to your work ethic and performance. Positive recommendations can open the door to flexible nursing shifts, per diem contracts, and specialized roles that pay more.
Flexibility is often rewarded in the world of contract nursing.
Consider these options to boost your pay:
- Accepting night shifts or weekends, which usually come with higher hourly rates.
- Taking assignments in locations experiencing shortages, such as rural facilities or emergency department nursing jobs.
- Being open to rapid response contracts or crisis response assignments, which often offer premium compensation.
When you demonstrate a willingness to adapt, you make yourself more valuable to medical staffing agencies and healthcare employers.
In contract nursing, your reputation follows you from one facility to the next. A strong track record makes it easier to secure higher-paying contracts and preferred assignments.
Tips for maintaining a great reputation:
- Be punctual and dependable.
- Communicate clearly with staffing agencies and supervisors.
- Go the extra mile to provide excellent patient care.
Facilities are willing to pay more to bring on nurses with proven reputations for excellence.
Being a contract nurse offers countless benefits, from career variety to premium pay. To make the most of your opportunities:
- Invest time in preparing a strong resume.
- Keep certifications and immunizations current.
- Maintain excellent references.
- Stay flexible with shifts and assignments.
- Build and protect your professional reputation.
When you combine preparation with dedication, you can consistently secure high-paying contract nursing jobs that match your skills and goals.
If you’re looking for your next opportunity, Staff Relief, Inc. is here to help. We partner with hospitals, clinics, and healthcare facilities to connect nurses with the best assignments in Georgia and beyond.
Contact us today to explore available contracts and start earning what you deserve.

Hiring More Nurses Generates Revenue for Hospitals
Underfunding is driving an acute shortage of trained nurses in hospitals and care facilities in the United States. It is the worst such shortage in more than four decades. One estimate from the American Hospital Association puts the deficit north of one million. Meanwhile, a recent survey by recruitment specialist AMN Healthcare suggests that 900,000 more nurses will drop out of the workforce by 2027.
American nurses are quitting in droves, thanks to low pay and burnout as understaffing increases individual workload. This is bad news for patient outcomes. Nurses are estimated to have eight times more routine contact with patients than physicians. They shoulder the bulk of all responsibility in terms of diagnostic data collection, treatment plans, and clinical reporting. As a result, understaffing is linked to a slew of serious problems, among them increased wait times for patients in care, post-operative infections, readmission rates, and patient mortality—all of which are on the rise across the U.S.
Tackling this crisis is challenging because of how nursing services are reimbursed. Most hospitals operate a payment system where services are paid for separately. Physician services are billed as separate line items, making them a revenue generator for the hospitals that employ them. But under Medicare, nursing services are charged as part of a fixed room and board fee, meaning that hospitals charge the same fee regardless of how many nurses are employed in the patient’s care. In this model, nurses end up on the other side of hospitals’ balance sheets: a labor expense rather than a source of income.
For beleaguered administrators looking to sustain quality of care while minimizing costs (and maximizing profits), hiring and retaining nursing staff has arguably become something of a zero-sum game in the U.S.
But might the balance sheet in fact be skewed in some way? Could there be potential financial losses attached to nurse understaffing that administrators should factor into their hiring and remuneration decisions?
Research by Goizueta Professors Diwas KC and Donald Lee, as well as recent Goizueta PhD graduates Hao Ding 24PhD (Auburn University) and Sokol Tushe 23PhD (Muma College of Business), would suggest there are. Their new peer-reviewed publication* finds that increasing a single nurse’s workload by just one patient creates a 17% service slowdown for all other patients under that nurse’s care. Looking at the data another way, having one additional nurse on duty during the busiest shift (typically between 7am and 7pm) speeds up emergency department work and frees up capacity to treat more patients such that hospitals could be looking at a major increase in revenue. The researchers calculate that this productivity gain could equate to a net increase of $470,000 per 10,000 patient visits—and savings to the tune of $160,000 in lost earnings for the same number of patients as wait times are reduced.
“A lot of the debate around nursing in the U.S. has focused on the loss of quality in care, which is hugely important,” says Diwas KC.
But looking at the crisis through a productivity lens means we’re also able to understand the very real economic value that nurses bring too: the revenue increases that come with capacity gains.Diwas KC, Goizueta Foundation Term Professor of Information Systems & Operations Management
“Our findings challenge the predominant thinking around nursing as a cost,” adds Lee. “What we see is that investing in nursing staff more than pays for itself in downstream financial benefits for hospitals. It is effectively a win-win-win for patients, nurses, and healthcare providers.”
To get to these findings, the researchers analyzed a high-resolution dataset on patient flow through a large U.S. teaching hospital. They looked at the real-time workloads of physicians and nurses working in the emergency department between April 2018 and March 2019, factoring in variables such as patient demographics and severity of complaint or illness. Tracking patients from admission to triage and on to treatment, the researchers were able to tease out the impact that the number of nurses and physicians on duty had on patient throughput. Using a novel machine learning technique developed at Goizueta by Lee, they were able to identify the effect of increasing or reducing the workforce. The contrast between physicians and nursing staff is stark, says Tushe.
“When you have fewer nurses on duty, capacity and patient throughput drops by an order of magnitude—far, far more than when reducing the number of doctors. Our results show that for every additional patient the nurse is responsible for, service speed falls by 17%. That compares to just 1.4% if you add one patient to the workload of an attending physician. In other words, nurses’ impact on productivity in the emergency department is more than eight times greater.”
Adding an additional nurse to the workforce, on the other hand, increases capacity appreciably. And as more patients are treated faster, hospitals can expect a concomitant uptick in revenue, says KC.
“It’s well documented that cutting down wait time equates to more patients treated and more income. Previous research shows that reducing service time by 15 minutes per 30,000 patient visits translates to $1.4 million in extra revenue for a hospital.”
In our study, we calculate that staffing one additional nurse in the 7am to 7pm emergency department shift reduces wait time by 23 minutes, so hospitals could be looking at an increase of $2.33 million per year.Diwas KC
This far eclipses the costs associated with hiring one additional nurse, says Lee.
“According to 2022 U.S. Bureau of Labor Statistics, the average nursing salary in the U.S. is $83,000. Fringe benefits account for an additional 50% of the base salary. The total cost of adding one nurse during the 7am to 7pm shift is $310,000 (for 2.5 full-time employees). When you do the math, it is clear. The net hospital gain is $2 million for the hospital in our study. Or $470,000 per 10,000 patient visits.”
These findings should provide compelling food for thought both to healthcare administrators and U.S. policymakers. For too long, the latter have fixated on the upstream costs, without exploring the downstream benefits of nursing services, say the researchers. Their study, the first to quantify the economic value of nurses in the U.S., asks “better questions,” argues Tushe; exploiting newly available data and analytics to reveal incontrovertible financial benefits that attach to hiring—and compensating—more nurses in American hospitals.
We know that a lot of nurses are leaving the profession not just because of cuts and burnout, but also because of lower pay. We would say to administrators struggling to hire talented nurses to review current wage offers, because our analysis suggests that the economic surplus from hiring more nurses could be readily applied to retention pay rises also.Sokol Tushe 23PhD, Muma College of Business
For state-level decision makers, Lee has additional words of advice.
“In 2004, California mandated minimum nurse-to-patient ratios in hospitals. Since then, six more states have added some form of minimum ratio requirement. The evidence is that this has been beneficial to patient outcomes and nurse job satisfaction. Our research now adds an economic dimension to the list of benefits as well. Ipso facto, policymakers ought to consider wider adoption of minimum nurse-to-patient ratios.”
However, decision makers go about tackling the shortage of nurses in the U.S., they should go about it fast and soon, says KC.
“This is a healthcare crisis that is only set to become more acute in the near future. As our demographics shift and our population starts again out, demand for quality will increase. So too must the supply of care capacity. But what we are seeing is the nursing staffing situation in the U.S. moving in the opposite direction. All of this is manifesting in the emergency department. That’s where wait times are getting longer, mistakes are being made, and overworked nurses are quitting. It is creating a vicious cycle that needs to be broken.”
Goizueta faculty apply their expertise and knowledge to solving problems that society—and the world—face. Learn more about faculty research at Goizueta.
*Ding, Tushe, Kc, Lee: “Frontiers in Operations: Valuing nursing productivity in emergency departments.” Manufacturing & Service Operations Management 26:4:1323-1337 (2024)

Georgia could see the largest shortage of RNs by 2036
Staffing is one of the biggest issues facing ASCs. A 2023 survey from ORManager found that in the last 12 months, 56% of ASCs reported an increase in volume. Despite this success, 68% of facilities also reported having a more difficult time recruiting experienced operating room nurses.
“I think the biggest threat towards ASCs in 2023 is staffing, especially qualified, experienced staffing in all areas of an ASC, including business office, pre-op, OR (both nursing and surgical technicians), post-anesthesia care unit and recovery nurses. In addition, sterile processing technicians,” Michael Powers, administrator of Knoxville, Tenn.-based Children’s West Surgery Center, told Becker’s. “Each of these areas require a certain set of skills that are acquired and honed over time. There is increased competition, and in fact it is hard to compete with large health systems/hospitals. I am also finding that ASCs are competing in the same region against one another for the available staffing pool.”
The HRSA report highlights nurse workforce projections from 2021 to 2036 generated using the agency’s health workforce simulation.
Here are the five states with the largest projected shortages of registered nurses by 2036, per the report:
1. Georgia: 29% projected shortage
Projected vacancies: 34,800
2. California: 26% projected shortage
Projected vacancies: 106,310
3. Washington: 26% projected shortage
Projected vacancies: 22,700
4. New Jersey: 25% projected shortage
Projected vacancies: 24,450
5. North Carolina: 23% projected shortage
Projected vacancies: 31,350
https://www.beckersasc.com/leadership/5-states-facing-the-biggest-nurse-shortages-by-2036
Breaking News
10 states with the most hospital closures, biggest net gains
A total of 743 general acute-care hospitals have closed across the United States since 2000, according to a July 22 news release from the Health Care Affordability Lab at Yale University in New Haven, Conn., and shared with Becker’s. The closure data is tracked through June 1, 2026. Hospital beds per 1,000 residents fell more than 20% over the period, from nearly three to just over two, and declined in every state.
The findings come from the Closures and Openings Explorer, a free interactive tool that tracks U.S. hospital changes from 2000 through June 2026 at the national, state, county and commuting-zone level. The dataset covers general, short-term, acute-care hospitals and excludes specialty facilities such as psychiatric, rehabilitation, children’s and VA hospitals. Researchers verified hospitals against state filings, financial statements, hospital websites and news reports, according to the release.
Hospital openings from 2024 forward were not tracked systematically and may be undercounted. The year 2000 served as the baseline, so hospitals already operating that year are not counted as openings. The state-by-state net-change figures below cover 2001 to 2023, the period for which both openings and closures are fully tracked, as well as total closures by state through June 2026.
“When we began this research, I expected to see more hospitals closing than opening. That’s true, but for every 10 hospitals that closed, eight opened. That surprised me,” Zack Cooper, PhD, director of the Health Care Affordability Lab at Yale, said in the release.
Here is the total number of hospital closures, by state, through June 2026, according to data from the tool shared with Becker’s:
States with the most hospital closures (2000 through June 2026):
- Texas: 98
- California: 64
- Pennsylvania: 54
- New York: 45
- Ohio: 31
- Tennessee: 26
- Georgia: 26
- Louisiana: 25
- Missouri: 25
- Alabama: 24
For the period in which both openings and closures are fully tracked, 2001 to 2023, 644 hospitals closed and 502 opened, for a net loss of 142. Twenty-nine states saw more closures than openings. Sixteen gained more hospitals than they lost. Five saw no net change. Here is how each state fared on net change, according to data shared with Becker’s:
States with the greatest net losses of hospitals (2001 to 2023):
- California: 62 closures, 21 openings, net -41
- New York: 41 closures, 2 openings, net -39
- Pennsylvania: 46 closures, 18 openings, net -28
- Georgia: 25 closures, 8 openings, net -17
- Michigan: 22 closures, 5 openings, net -17
- New Jersey: 16 closures, 1 opening, net -15
- Tennessee: 23 closures, 9 openings, net -14
- Illinois: 18 closures, 5 openings, net -13
- Missouri: 20 closures, 7 openings, net -13
- Alabama: 17 closures, 6 openings, net -11
States with the greatest net gains of hospitals (2001 to 2023):
- Texas: 131 openings, 91 closures, net +40
- Colorado: 17 openings, 2 closures, net +15
- Arizona: 23 openings, 11 closures, net +12
- Florida: 32 openings, 21 closures, net +11
- Nevada: 13 openings, 2 closures, net +11
- Wisconsin: 15 openings, 5 closures, net +10
- Utah: 8 openings, 0 closures, net +8
- New Mexico: 8 openings, 3 closures, net +5
- Washington: 9 openings, 4 closures, net +5
- Wyoming: 5 openings, 0 closures, net +5
States with no net change (2001-2023): Connecticut, Idaho, Nebraska, New Hampshire, Vermont.
Explore the data here.
The post 10 states with the most hospital closures, biggest net gains appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
10 fastest-growing large cities for jobs: LinkedIn
San Francisco is the fastest-growing large U.S. city for jobs and talent, according to a July 22 list from LinkedIn News.
It was created by identifying the U.S. cities with the strongest job market momentum and net positive migration, focusing on areas with more than 2.5 million LinkedIn members.
Dallas and Orlando, Fla., broke into the top 10 in the latest edition, fueled by job growth in industries including healthcare, according to LinkedIn News.
Here are the 10 fastest-growing large U.S. cities for jobs and talent, per LinkedIn:
1. San Francisco
2. Minneapolis
3. New York City
4. Seattle
5. Chicago
6. Dallas
7. Orlando, Fla.
8. Miami
9. Atlanta
10. Denver
The post 10 fastest-growing large cities for jobs: LinkedIn appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
1 in 4 US workers stay in jobs for health insurance: Gallup
Nearly 1 in 4 U.S. workers (24%), the equivalent of about 23 million adults, are staying in jobs they want to leave to keep their employer-sponsored health insurance, according to a July 21 report from the West Health-Gallup Center on Healthcare in America. The share marks an 8-percentage-point rise since 2021, when 16% of workers reported the same.
The findings come from a nationally representative study of 5,660 U.S. adults conducted Oct. 27 to Dec. 22, 2025, on the Gallup Panel. The analysis focuses on 2,322 respondents who are employed and rely on employer-sponsored coverage as their primary insurance.
The report identifies several groups with elevated rates of job lock. Workers who report household medical debt they will be unable to repay in the next 12 months were more than twice as likely to report staying in unwanted jobs for insurance (44%) compared with those without such debt (21%). Workers with three or more chronic conditions reported the highest rate of any subgroup, at 41%. Women reported job lock at 30%, compared with 20% for men.
The rise in job lock tracks alongside broader healthcare affordability strain. About half of Americans report difficulty consistently paying for needed medical care or prescriptions, and 51% said they were worried about their ability to afford healthcare over the next 12 months, the highest level in five years, according to a separate West Health-Gallup measure cited in the report.
The post 1 in 4 US workers stay in jobs for health insurance: Gallup appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
States ranked by ED physicians per capita
Emergency medicine physicians per capita vary more than fourfold across the U.S., from 51.32 per 100,000 residents in the District of Columbia to 11.55 in Alabama, according to data from KFF and the U.S. Census Bureau.
Becker’s used KFF’s count of professionally active emergency medicine physicians, sourced from Redi-Data as of May, and calculated per capita rates using the latest Census Bureau state population estimates. Totals were found by dividing each state’s total ED physicians by its population and multiplying by 100,000.
Washington, D.C. topped the list by a wide margin, at 51.32 ED physicians per 100,000 residents — about 20 points ahead of second-place Michigan. The gap is likely a denominator effect rather than a staffing story: the capital’s small resident population (about 690,000) sits alongside a dense cluster of academic medical centers and regional referral hospitals that serve a much larger regional patient base than the resident count reflects.
Nationwide, there are 67,617 professionally active emergency medicine physicians, or 19.78 per 100,000 residents.
Here are states ranked by number of ED physicians per 100,000 residents.
| State | Total employed physicians | Physicians per 100,000 residents |
| District of Columbia | 356 | 51.32 |
| Michigan | 3141 | 31.01 |
| Rhode Island | 342 | 30.69 |
| Vermont | 181 | 28.08 |
| Alaska | 202 | 27.40 |
| Hawaii | 385 | 26.87 |
| Maine | 372 | 26.29 |
| Ohio | 3012 | 25.31 |
| Massachusetts | 1803 | 25.20 |
| Pennsylvania | 3259 | 24.96 |
| Oregon | 1030 | 24.10 |
| New York | 4795 | 23.97 |
| Connecticut | 884 | 23.97 |
| Delaware | 253 | 23.87 |
| Wyoming | 134 | 22.76 |
| New Mexico | 475 | 22.35 |
| New Hampshire | 316 | 22.33 |
| Colorado | 1318 | 21.92 |
| Missouri | 1374 | 21.91 |
| Illinois | 2777 | 21.83 |
| West Virginia | 367 | 20.78 |
| Wisconsin | 1227 | 20.54 |
| South Carolina | 1111 | 19.95 |
| Montana | 227 | 19.83 |
| Minnesota | 1150 | 19.72 |
| Virginia | 1738 | 19.57 |
| California | 7682 | 19.52 |
| New Jersey | 1836 | 19.23 |
| Arizona | 1443 | 18.93 |
| Florida | 4406 | 18.78 |
| Washington | 1479 | 18.49 |
| Louisiana | 834 | 18.06 |
| Oklahoma | 742 | 18.00 |
| Maryland | 1127 | 17.99 |
| Nevada | 590 | 17.98 |
| North Carolina | 2007 | 17.92 |
| Utah | 592 | 16.73 |
| Kentucky | 765 | 16.61 |
| Indiana | 1110 | 15.92 |
| Mississippi | 466 | 15.77 |
| Georgia | 1775 | 15.70 |
| Texas | 4824 | 15.21 |
| North Dakota | 115 | 14.39 |
| Tennessee | 1050 | 14.35 |
| Nebraska | 289 | 14.32 |
| Idaho | 285 | 14.04 |
| Iowa | 435 | 13.43 |
| Arkansas | 416 | 13.36 |
| Kansas | 396 | 13.30 |
| South Dakota | 124 | 13.26 |
| Alabama | 600 | 11.55 |
The post States ranked by ED physicians per capita appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
States ranked by surgeons per capita
The District of Columbia has the highest concentration of general surgeons in the U.S., with 71.79 general surgeons per capita, according to a Becker’s analysis of state-level general surgeon counts from KFF and 2025 U.S. population estimates.
Idaho has the lowest concentration of general surgeons per capita at 9.66.
The number of general surgeons per 100,000 residents was calculated by dividing the total number of general surgeons in each state by that state’s total population, then multiplying the result by 100,000.
Here are the states, ranked by number of general surgeons per 100,000 residents:
| State | Total general surgeons | General surgeons per capita |
| District of Columbia | 498 | 71.79 |
| New York | 5,505 | 27.52 |
| Massachusetts | 1,960 | 27.40 |
| Connecticut | 990 | 26.84 |
| North Dakota | 184 | 23.02 |
| Rhode Island | 254 | 22.79 |
| Maryland | 1,364 | 21.77 |
| Ohio | 2,546 | 21.39 |
| Pennsylvania | 2,764 | 21.16 |
| New Mexico | 446 | 20.98 |
| Michigan | 2,124 | 20.97 |
| Maine | 284 | 20.07 |
| New Hampshire | 277 | 19.57 |
| Vermont | 126 | 19.55 |
| South Dakota | 176 | 18.82 |
| New Jersey | 1,712 | 17.93 |
| Minnesota | 1,032 | 17.70 |
| Nebraska | 357 | 17.69 |
| Oregon | 742 | 17.36 |
| West Virginia | 302 | 17.10 |
| Kentucky | 786 | 17.06 |
| Wisconsin | 1,012 | 16.94 |
| Missouri | 1,050 | 16.74 |
| Louisiana | 763 | 16.52 |
| Tennessee | 1,194 | 16.32 |
| North Carolina | 1,816 | 16.22 |
| Florida | 3,748 | 15.97 |
| Arizona | 1,153 | 15.12 |
| Delaware | 160 | 15.10 |
| Hawaii | 216 | 15.08 |
| California | 5,908 | 15.01 |
| Alaska | 110 | 14.92 |
| Illinois | 1,863 | 14.65 |
| Virginia | 1,297 | 14.61 |
| Iowa | 471 | 14.54 |
| Alabama | 755 | 14.54 |
| Colorado | 871 | 14.49 |
| Kansas | 430 | 14.44 |
| Washington | 1,136 | 14.20 |
| Georgia | 1,594 | 14.10 |
| Arkansas | 439 | 14.09 |
| South Carolina | 782 | 14.04 |
| Montana | 160 | 13.98 |
| Wyoming | 78 | 13.25 |
| Indiana | 917 | 13.15 |
| Texas | 4,117 | 12.98 |
| Mississippi | 368 | 12.46 |
| Nevada | 360 | 10.97 |
| Oklahoma | 443 | 10.74 |
| Utah | 374 | 10.57 |
| Idaho | 196 | 9.66 |
The post States ranked by surgeons per capita appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
10 best, worst cities for renters
Scottsdale, Ariz., is the best place in the U.S. to rent, largely because of its quality of life, according to a July 7 ranking from personal finance website WalletHub.
To develop the list of the best local rental markets, WalletHub compared 182 U.S. cities, including the 150 most populated and at least two of the most populated from each state. It evaluated 21 metrics across rental market and affordability and quality of life, including rental affordability, cost of living, job market and safety.
As many U.S. cities face rising housing costs, health systems have taken employee housing into their own hands to ensure recruitment and retention. One example is Atlanta-based Emory University, which is renovating two buildings to house staff at Emory Healthcare. It will create more than 50 rental apartments for staff whose salaries fall within specific levels.
Here are the 10 best and worst places to rent in the U.S., per WalletHub:
Best
1. Scottsdale, Ariz.
2. Gilbert, Ariz.
3. Chandler, Ariz.
4. Overland Park, Kan.
5. Columbia, Md.
6. Peoria, Ariz.
7. Bismarck, N.D.
8. Huntsville, Ala.
9. Sioux Falls, S.D.
10. Amarillo, Texas
Worst
173. Shreveport, La.
174. Huntington, W.Va.
175. Augusta, Ga.
176. New Orleans
177. Newark, N.J.
178. Akron, Ohio
179. Memphis, Tenn.
180. Jackson, Miss.
181. Cleveland
182. Detroit
The post 10 best, worst cities for renters appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
States with the most, fewest physicians per capita
The District of Columbia, New York and Massachusetts have the most physicians per capita, while Mississippi, Alabama and Nevada have the fewest, according to Bureau of Labor statistics and Census data.
Becker’s used the bureau’s latest data — 2025 statistics — to find the total number of physicians and used Census data to calculate the number of physicians per capita using state population totals in 2025. Becker’s then used the bureau’s and Census data to also find the physicians per capita for 2024.
Nationwide, there were 754,760 employed physicians in 2025, up from 717,900 in 2024. Between 2024 and 2025, Arkansas and Alaska had the highest increase in physicians per capita, while Mississippi and Wyoming had the largest cut in physicians per capita.
Here are the total employed physicians, along with the physicians per capita in 2025 and the percent change in physicians per capita compared to 2024.
| State | Total employed physicians | Physicians per capita in 2025 | Percent change compared to physicians per capita in 2024 |
| Alabama | 5,350 | 103.02 | -9.02% |
| Alaska | 1,800 | 244.14 | 24.62% |
| Arizona | 14,630 | 191.90 | 4.98% |
| Arkansas | 6,390 | 205.15 | 43.02% |
| California | 55,790 | 141.76 | -21.37% |
| Colorado | 9,280 | 154.34 | -3.11% |
| Connecticut | 10,020 | 271.66 | 2.71% |
| Delaware | 2,840 | 267.94 | 0.66% |
| District of Columbia | 3,470 | 500.26 | -17.34% |
| Florida | 41,530 | 177.01 | -6.55% |
| Georgia | 21,920 | 193.94 | -7.53% |
| Hawaii | 3,910 | 272.89 | 14.06% |
| Idaho | 3,300 | 162.58 | 18.77% |
| Illinois | 32,000 | 251.59 | 7.56% |
| Indiana | 17,850 | 255.98 | 17.54% |
| Iowa | 5,050 | 155.94 | 4.22% |
| Kansas | 6,330 | 212.61 | 14.01% |
| Kentucky | 8,800 | 191.02 | 3.48% |
| Louisiana | 6,870 | 148.76 | +0.73% |
| Maine | 3,710 | 262.21 | -0.70% |
| Maryland | 17,360 | 277.08 | -7.69% |
| Massachusetts | 21,370 | 298.71 | -7.60% |
| Michigan | 25,690 | 253.66 | -5.74% |
| Minnesota | 16,910 | 290.03 | 9.53% |
| Mississippi | 1,950 | 66.01 | -41.49% |
| Missouri | 9,220 | 147.04 | -8.63% |
| Montana | 1,340 | 117.06 | -3.54% |
| Nebraska | 5,080 | 251.73 | 13.70% |
| Nevada | 3,720 | 113.34 | -8.56% |
| New Hampshire | 3,750 | 264.95 | -1.50% |
| New Jersey | 21,330 | 223.39 | -3.04% |
| New Mexico | 3,760 | 176.90 | -2.37% |
| New York | 70,670 | 353.31 | 17.56% |
| North Carolina | 23,600 | 210.75 | 6.54% |
| North Dakota | 1,950 | 243.95 | 9.79% |
| Ohio | 34,610 | 290.83 | -2.34% |
| Oklahoma | 6,010 | 145.76 | 5.47% |
| Oregon | 9,990 | 233.76 | -8.88% |
| Pennsylvania | 34,960 | 267.70 | 7.33% |
| Rhode Island | 2,890 | 259.30 | 2.64% |
| South Carolina | 9,680 | 173.78 | -0.92% |
| South Dakota | 1,830 | 195.70 | -0.03% |
| Tennessee | 13,100 | 179.08 | -5.31% |
| Texas | 60,080 | 189.47 | 3.36% |
| Utah | 6,100 | 172.37 | -2.91% |
| Vermont | 1,730 | 268.36 | -8.89% |
| Virginia | 15,660 | 176.35 | 5.63% |
| Washington | 14,390 | 179.85 | -2.17% |
| West Virginia | 4,390 | 248.56 | 12.23% |
| Wisconsin | 15,360 | 257.17 | 9.58% |
| Wyoming | 760 | 129.09 | -24.15% |
The post States with the most, fewest physicians per capita appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Nurse practitioner workforce growth to far outpace physicians, physician assistants: Study
The nurse practitioner workforce is projected to grow 11% annually through 2030, far outpacing projected growth for physician assistants and physicians, according to workforce estimates published in Health Affairs.
Researchers from Columbia University, Brandeis University, George Washington University and New York University forecast physician supply will continue growing about 1% annually through 2030, while physician assistant supply is projected to grow 5.6% annually. By 2030, the combined number of nurse practitioners and physician assistants is expected to approach the size of the physician workforce, with an estimated 912,265 clinicians, compared with 1,068,016 physicians. The estimates are based on U.S. Census Bureau American Community Survey data through 2023.
The authors said the projections are higher than previous federal estimates from the Health Resources and Services Administration because they incorporate more recent workforce trends, particularly the rapid expansion of younger nurse practitioners entering the profession.
Researchers said the differing growth rates are largely driven by accelerated growth among nurse practitioners younger than 40 years old compared with slower growth among physician assistants in the same age group.
“As the U.S. population ages and demand for care grows, NPs and PAs are well positioned to fill critical gaps, and newly graduated NPs will constitute a rapidly growing share of the workforce in the near term,” the authors wrote. “Health systems that invest now in onboarding, interprofessional training and team-based care models will be better prepared to capitalize on the opportunities and manage the transitions that accompany this workforce evolution.”
The authors also said policymakers should ensure regulations and payment policies “more effectively leverage this growing workforce to address geographic and specialty shortages.”
The researchers noted several limitations. The projections assume recent workforce trends continue and do not account for future policy changes, economic shifts or changes in education capacity that could affect clinician supply. They also rely on self-reported Census Bureau survey data and measure workforce size rather than clinical hours worked or specialty distribution.
The post Nurse practitioner workforce growth to far outpace physicians, physician assistants: Study appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Nurse AI adoption outpaces hospital strategy: Survey
Nurse AI adoption is accelerating faster than hospitals are building strategies to support it, a report from Incredible Health found.
Healthcare staffing company Incredible Health released its 2026 Annual State of Nursing report July 7. The findings are based on a national survey of 2,240 U.S. nurses. The report also incorporates platform data from Incredible Health’s network of 1.5 million U.S. healthcare professionals. The full report is accessible from Incredible Health here.
Here are six key findings from the report:
- Forty-four percent of nurses now use AI at work, up from 15% a year earlier.
- Many nurses reported receiving little formal preparation to use AI tools. Forty-six percent said they received no AI training in the past year, while 5% said they received formal training that adequately prepared them.
- Among nurses who use AI, the most common applications were documentation and charting (37%), creating patient education materials (37%) and drug or clinical reference lookups (32%).
- Nurses who received AI training were more likely to report saving more than an hour per day using the technology than nurses who did not receive training (24% versus 16%). At the same time, half of AI users said their most recent use of AI saved little or no time.
- The survey also found nurses who were involved in selecting AI tools were more likely to use them than those who were not consulted. Eighty-one percent of nurses who helped choose AI tools reported using them, compared with 62% of nurses who were never consulted.
- One in five nurses said AI tools “just appear” in their workplace without a plan or explanation, and only 17% of nurses working in organizations that already use AI said their employer’s strategy for the technology is clear.
The post Nurse AI adoption outpaces hospital strategy: Survey appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
23% of organizations are not prioritizing clinician burnout: Poll
Among organizations, 23% said clinician burnout is not a current focus, compared to 17% that reported its their No. 1 concern.
In a LinkedIn poll, Becker’s asked, “Where does clinician burnout rank among your organization’s top operational concerns heading into the second half of 2026?”
The poll received 323 votes and was conducted June 23. Becker’s does not have insights on the respondents’ organizations or roles.
The results:
No. 1 — it’s our top worry: 17%
In our top 3: 43%
Higher vs. last year: 17%
Not a current focus: 23%
The post 23% of organizations are not prioritizing clinician burnout: Poll appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
The Most Underrated Workforce Lever in Health Systems
Health systems are paying twice for the same clinical talent. Most have not figured that out yet.
At large academic medical centers, hundreds of clinical students rotate through hospitals and outpatient sites every year. They work beside nurses, therapists, and pharmacists. They are evaluated daily by preceptors who form fast, accurate judgments about who they would hire. Most of those students do eventually get hired somewhere. Usually not where they trained.
That pattern repeats across nearly every health system in the country. It is one of the most expensive inefficiencies in clinical workforce strategy, and it is hiding in plain sight. Health systems like Valley Health and Sarah Bush Lincoln have started to address it. What they found reveals a structural gap most organizations have not examined.
The investment is already being made
Health systems are not passive participants in clinical education. Preceptors carry real supervisory load. Coordinators manage placement logistics across dozens of school partners. Compliance teams verify documentation. Departments absorb the productivity cost of training students in live care environments.
That investment produces something a job interview simply cannot replicate: weeks of real-environment evaluation across clinical judgment, communication, coachability, and culture fit. The signal is there. The question is whether it ever reaches a hiring decision.
For most health systems, it does not. Students complete rotations, graduate, and enter the open job market. The health system that trained them often reconnects only after paying agency premiums to fill the same role.
The NSI 2025 National Health Care Retention and RN Staffing Report puts the average cost of turnover for a bedside RN at $61,110, with each percentage point change in RN turnover costing the average hospital an additional $289,000 per year. When you hold that number up against the cost of training a clinician, losing them to the open market, and paying to recruit a replacement, the math becomes hard to ignore.
Where the breakdown actually happens
The problem sits between two functions that almost never share infrastructure. Clinical education manages student placements, preceptors, and school relationships. Talent acquisition manages requisitions and pipelines. Both teams directly shape workforce outcomes but neither typically has visibility into what the other is doing.
A student who performs well on rotation, expresses interest in employment, and earns strong feedback from a preceptor can still fall completely out of view. The preceptor’s evaluation lives in a hallway conversation. The student’s interest sits in a survey or an email. No one has a consolidated picture of which rotation sites, departments, or school partners are consistently producing strong future hires.
What looks like missed recruitment is also operational drag: coordinators spend the majority of their time on manual placement tracking, document chasing, and reconciling school-specific intake processes. Compliance gets managed reactively, creating last-minute delays and audit exposure. Capacity decisions get made on instinct because real-time visibility across departments and locations does not exist. And preceptor intelligence about student quality disappears at the end of every rotation.
The intent to hire from rotations is already there. “We see every rotation as a two-way interview,” says Tracey McCord, MSN, RN, NPD-BC, Professional Development Coordinator at Sarah Bush Lincoln Health System. “We’re evaluating students, and they’re evaluating us. We want them to leave thinking: this is where I want to work. They are our future workforce, and we’ve always known that.” That belief is common across health systems. The infrastructure to act on it is not.
A different way to operate
A small number of health systems have started treating clinical education as workforce infrastructure rather than an administrative function. The shift shows up in how the work is organized.
Placement coordination runs through a single system across disciplines, locations, and school partners. Compliance is enforced before day one, with audit-ready records available on demand. Preceptor evaluations attach to the student record and travel with it. Leadership sees capacity, demand, and onboarding completion in real time. And rotation performance feeds directly into hiring conversations through a structured pipeline.
At Valley Health, one person manages close to 1,500 students a year. Halle Esparza, Academic Services Coordinator, coordinates rotations across six hospitals, 188 locations, and 25 disciplines. In 2025, that meant 1,859 coordinated placements. Getting to that scale required infrastructure. And infrastructure is what makes a hiring pipeline possible, because you cannot track which students you want to hire if you cannot track which students are in the building.
The Maryland-DC Nursing Collaborative coordinates roughly 25,000 nursing placements a year across more than 30 hospitals and 30 schools on a shared platform. That kind of scale is not operationally feasible without standardized infrastructure underneath it.
The organizations that have made this shift describe the same pattern consistently. Coordinator hours redirect from data entry to student experience. Compliance exposure drops. And workforce planning gets earlier and sharper because rotation data is finally legible at the leadership level.
The takeaway
Workforce shortages will not be solved through external recruiting alone. Clinical rotation programs are generating pipeline-ready candidates and decision-grade workforce intelligence every single day. Most health systems are not equipped to capture any of it.
McCord speaks for clinical education leaders at health systems across the country: “They are our future workforce, and we’ve always known that.” The health systems that have stopped paying twice for that future built the infrastructure to identify, develop, and recruit their best rotation students before a competitor did.
Valley Health, Sarah Bush Lincoln Health System, and the Maryland-DC Nursing Collaborative all run on Exxat One. So do health systems and consortiums across the country working to close the gap between placement and pipeline.
The most underrated workforce lever in health systems may have been in the building the whole time.
Learn more about Exxat One here.
The post The Most Underrated Workforce Lever in Health Systems appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
The discipline helping rural hospitals survive
At least 15 rural hospitals have closed in the last year. Hundreds more are operating under sustained financial pressure from Medicaid cuts, reimbursement gaps and a workforce market that increasingly tilts toward larger systems. For the executives running small community hospitals, financial survival has become a daily discipline requiring thoughtful decision-making.
Justin Harris, became CEO of Daviess Community Hospital in Washington, Ind., in July 2025. The most consequential decision of his first year in the role was a partnership choice. The hospital had operated under a management agreement since 2017 and when Mr. Harris took the helm, Daviess Community entered a new arrangement with Evansville, Ind.-based Deaconess Health System — a regional operator whose model, is built explicitly around keeping care in the communities it serves rather than routing patients toward larger tertiary centers. Within roughly six months, the hospital shifted from losing millions of dollars each month to posting positive margins.
“That takes partnership, that takes commitment to the community, that takes involvement from the community,” Mr. Harris said. “And that is exactly what we’re doing at Daviess Community Hospital.”
The revenue cycle is ground no executive can afford to cede. Mr. Harris was direct about the personal role he believes leaders at every level must play.
“You are never too big to not be involved in the revenue cycle,” he said. “We need to be in our financials and revenue cycle, and we need to make decisions on a daily basis about how to lead the organization.”
He described recoupments, readmissions and pre-authorizations as executive responsibilities rather than back-office concerns.
“If we don’t make any money, it’s hard to provide good healthcare,” Mr. Harris said. “You don’t have the ability to bring services, you don’t have the ability to buy supplies, pay your staff.”
Eric Price, CFO of Schoolcraft Memorial Hospital in Manistique, Mich., arrived at the same conclusion. He watched successive waves of regulatory urgency — ICD-10, ACA implementation, the current rural transformation funding debates — generate intense pressure that generally resolves within months. For a 12-bed critical access hospital, chasing each one carries a cost in leadership bandwidth and organizational focus that small teams cannot easily absorb.
“The initial surge of information will usually resolve itself,” he said. “In six to eight months, things tend to settle down.”
That long view shapes how Schoolcraft evaluates any significant initiative. Mr. Price asks where a strategy will stand five or 10 years in the future and then collaborates with his team on the best path forward. The initiatives that can’t hold up under that question don’t command the organization’s attention.
“We’ve got to maintain that long-term strategy,” he said. “I’m hoping to come back here in five years and say, hey — we weathered that storm, and now we’re done with this new one.”
In practice, that also means staying anchored to patient care when financial pressures are pulling in multiple directions.
“The most decisive thing we’ve done is ensuring that among all the change we don’t lose sight of patient quality care,” said Mr. Price. “The fact that at the end of the day, especially in rural America, it’s our family members. It’s our mothers, our neighbors, people we grew up with and we’ll see them on the street and at the grocery store. We’ve got to stay focused on patient care and not lose sight of quality and access.”
He is equally clear that financial leadership demands physical presence in the building. A CFO who manages from a spreadsheet is ineffective.
“If you’re sitting at your desk, you’re not rounding on the med-surg unit, checking in on your OR team, having conversations with physicians, you may be a little behind the power curve already,” he said. “I need to know what’s going on so I can react effectively.”
JohnRich Levin, chief nursing officer at Reeves Regional Health in Pecos, Texas, relies on operational simplicity to weather storms. Reeves Regional is a critical access hospital in West Texas where the nearest major city is an hour and a half away. In that environment, complexity becomes a liability.
He described the limits of predictive analytics in a setting built on personal, direct knowledge of the patient population.
“You can’t be too complicated in a rural facility,” he said. “We have this AI technology, and we have all these things going on. And yet, we know that much of them don’t really apply until we actually desperately really need them. How do you apply predictive analytics when you know who your patients are and you actually know when they are not showing up and you wonder what’s going on with them? There’s nothing that could be replaced by human interaction.”
His emphasis is on workforce development, building the clinical versatility and leadership competency that a small team needs when backup is not nearby. The move from 20 years at a large Houston facility to rural West Texas reinforced a lesson Mr. Levin now applies at Reeves Regional: headcount and readiness are not the same thing.
“You’ve got to assess the kind of staff that you have and build them from there,” Mr. Levin said.
Across all three accounts, culture emerged as the variable that determines whether financial improvements hold. Operations and margins can shift relatively quickly under disciplined leadership. Whether those gains last is harder to influence.
“We can change our operations and financials, and sometimes pretty quickly,” Mr. Harris said. “But if your team is not on board, if your medical staff is not on board, then it’s hard to make that last and be sustainable.”
The post The discipline helping rural hospitals survive appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
20 most, least health stressed US cities
Fremont, Calif., ranks as the city with the lowest health and safety stress, while Memphis, Tenn., is the most stressed, WalletHub found.
WalletHub compared 182 cities, including the 150 most populated U.S. cities plus at least two of the most populated cities in each state. Each city was compared across 39 metrics in four dimensions: work stress, financial stress, family stress, and health and safety stress. Each metric was graded on a 100-point scale, with 100 representing the highest level of stress.
In health stress, the report tracked the percentage of adults in fair or poor health and found a three times difference between the worst and best cities for this metric. Four cities tied for the highest percentage of adults in fair/poor health: San Antonio, Texas; Louisville, Ky.; Shreveport, La.; Brownsville, Texas. The city with the lowest percentage was Cheyenne, Wyo.
Here are the cities with the highest and lowest health and safety stress, along with their total stress score.
Most stressed in health and safety
- Memphis, Tenn.: 59.24
- Detroit, Mich.: 62.78
- Shreveport, La.: 57.75
- Cleveland, Ohio: 59.35
- Huntington, W.Va.: 50.32
- Charleston, W.Va.: 45.97
- Gulfport, Miss.: 56.90
- Houston, Texas: 54.18
- Dover, Del.: 49.86
- Jackson, Miss.: 56.03
- Birmingham, Ala.: 54.42
- Springfield, Mo.: 44.07
- St. Louis, Mo.: 54.60
- Augusta, Ga.: 50.37
- Kansas City, Mo.: 44.67
- Knoxville, Tenn.: 43.98
- San Antonio, Texas: 51.37
- Montgomery, Ala.: 52.59
- Fort Smith, Ark.: 48.55
- Baton Rouge, La.: 52.95
Least stressed
- Fremont, Calif.: 26.16
- Irvine, Calif.: 31.06
- San Francisco, Calif.: 36.75
- Jersey City, N.J.: 36.25
- San Jose, Calif.: 31.48
- Columbia, Md.: 35.21
- Overland Park, Kan.: 30.83
- South Burlington, Vt.: 26.22
- San Diego, Calif.: 35.70
- Chula Vista, Calif.: 38.09
- Santa Clarita, Calif.: 39.45
- Scottsdale, Ariz.: 36.17
- Gilbert, Ariz.: 34.09
- Chandler, Ariz.: 35.88
- Yonkers, N.Y.: 37.93
- Burlington, Vt.: 31.62
- Raleigh, N.C.: 37.26
- Huntington Beach, Calif.: 37.28
- Madison, Wis.: 32.80
- Garden Grove, Calif.: 38.99
The post 20 most, least health stressed US cities appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Nursing home workforce adds 3,300 jobs in June amid deportation, shortage concerns
The nursing home workforce gained 3,300 jobs in June, bringing the total number of workers up to 1,586,600, the American Health Care Association said in a July 6 news release shared with Becker’s.
The association used the Bureau of Labor Statistics to find current nursing home workforce statistics. Here is what to know about the current state of the workforce:
1. Both nursing home staff turnover and temporary staff agency use have declined since 2022.
2. Nursing home and residential care facilities’ staffing is rebounding. Since the pandemic, the number of workers in nursing facilities has steadily risen. As of May, the industry employs about 3.49 million people, up from 2.96 million at the industry’s lowest point in January 2022.
3. On June 25, the Supreme Court ended Temporary Protected Status for Haitian and Syrian citizens, clearing the way for the federal government to deport hundreds of thousands of workers. The ruling puts more than 330,000 Haitians and more than 6,000 Syrians at risk of deportation, Americans for Immigrant Justice said. The nursing home industry relies heavily on immigrant labor, which makes up about 28% of the long-term care workforce.
4. By 2030, all 73 million Baby Boomers will be at least 65 years old. Meanwhile, a growing shortage of registered nurses and licensed practical nurses is projected by 2038.
The post Nursing home workforce adds 3,300 jobs in June amid deportation, shortage concerns appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
60 statistics on hospital expenses in mid-2026
For years, labor dominated the hospital expense conversation. Staffing shortages, travel nurse premiums and wage competition consumed the attention of CFOs and operations leaders across the country. Recent data from Kaufman Hall shows times have changed.
Labor costs have stabilized into a relatively predictable range while drugs, supplies, purchased services and more have become the harder problem to solve.
Drug and non-labor expenses are now growing faster than labor in nearly every region and at nearly every hospital size, and unlike labor costs, they offer fewer obvious levers for management to pull. Labor expense growth is holding in a relatively tight band across the industry, roughly 3% to 5% year-over-year regardless of geography or bed size.
Non-labor and drug expenses show no such consistency. Double-digit increases represent a structural shift in where financial pressure is originating.
The geographic divergence is also worth noting. Hospitals in the South are managing the most balanced expense profile, with all five major categories growing at roughly the same pace. The West and Midwest face a materially different picture, with non-labor and drug costs accelerating well above the national average. For health system leaders operating across multiple regions, that divergence complicates any systemwide cost management strategy.
What the data cannot capture, but what CFOs understand acutely, is that this expense growth is arriving alongside worsening payer mix. Bad debt and charity care are rising year-over-year across every region and bed size, meaning hospitals are absorbing higher costs while simultaneously collecting less on the revenue side. Expense growth that might be manageable in a stable reimbursement environment becomes significantly more threatening when the payer mix is eroding at the same time.
Here are 60 statistics on hospital expense growth based on Kaufman Hall’s National Hospital Flash Report, which includes data from 1,300-plus hospitals gathered by Strata Decision Technology.
Overall national trends (year-over-year, April 2026 vs. April 2025)
1. Total expense per calendar day: +7%
2. Labor expense per calendar day: +4%
3. Non-labor expense per calendar day: +9%
4. Drug expense per calendar day: +9%
5. Purchased service expense per calendar day: +4%
By region (year-over-year, April 2026 vs. April 2025)
West
6. Total expense per calendar day: +9%
7. Labor expense per calendar day: +5%
6. Non-labor expense per calendar day: +13%
9. Drug expense per calendar day: +17%
10. Purchased service expense per calendar day: +8%
Midwest
11. Total expense per calendar day: +8%
12. Labor expense per calendar day: +3%
13. Non-labor expense per calendar day: +10%
14. Drug expense per calendar day: +9%
15. Purchased service expense per calendar day: +5%
South
16. Total expense per calendar day: +6%
17. Labor expense per calendar day: +6%
18. Non-labor expense per calendar day: +6%
19. Drug expense per calendar day: +9%
20. Purchased service expense per calendar day: +2%
Northeast / Mid-Atlantic
21. Total expense per calendar day: +6%
22. Labor expense per calendar day: +4%
23. Non-labor expense per calendar day: +11%
24. Drug expense per calendar day: +8%
25. Purchased service expense per calendar day: +1%
Great Plains
26. Total expense per calendar day: +5%
27. Labor expense per calendar day: +3%
28. Non-labor expense per calendar day: +9%
29. Drug expense per calendar day: +11%
30. Purchased service expense per calendar day: +5%
By hospital bed size (year-over-year, April 2026 vs. April 2025)
0-25 beds
31. Total expense per calendar day: +6.1%
32. Labor expense per calendar day: +3.0%
33. Non-labor expense per calendar day: +7.7%
34. Drug expense per calendar day: -0.6%
35. Purchased service expense per calendar day: +2.1%
26-99 beds
36. Total expense per calendar day: +7.4%
37. Labor expense per calendar day: +4.2%
38. Non-labor expense per calendar day: +9.8%
39. Drug expense per calendar day: +10.5%
40. Purchased service expense per calendar day: +1.4%
100-199 beds
41. Total expense per calendar day: +8.0%
42. Labor expense per calendar day: +4.3%
43. Non-labor expense per calendar day: +9.4%
44. Drug expense per calendar day: +9.1%
45. Purchased service expense per calendar day: +8.1%
200-299 beds
46. Total expense per calendar day: +5.1%
47. Labor expense per calendar day: +4.5%
48. Non-labor expense per calendar day: +7.7%
49. Drug expense per calendar day: +13.6%
50. Purchased service expense per calendar day: +5.0%
51. Total expense per calendar day: +8.0%
300-499 beds
52. Labor expense per calendar day: +4.8%
53. Non-labor expense per calendar day: +10.4%
54. Drug expense per calendar day: +9.8%
55. Purchased service expense per calendar day: +5.2%
500+ beds
56. Total expense per calendar day: +6.6%
57. Labor expense per calendar day: +4.0%
58. Non-labor expense per calendar day: +9.2%
59. Drug expense per calendar day: +13.5%
60. Purchased service expense per calendar day: +1.1%
The post 60 statistics on hospital expenses in mid-2026 appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Healthcare job growth slows to 21,500 in June: 4 things to know
Healthcare added 21,500 jobs in June, slowing down from the average monthly gain of 38,000 over the past year, according to the U.S. Bureau of Labor Statistics.
Here are four things to know from the July 2 jobs report:
1. Hospitals added 9,200 jobs in June, up from a revised 6,800 in May.
2. Ambulatory healthcare services added 8,000 jobs, including 3,300 in home health care.
3. Nursing and residential care facilities added 4,300 jobs.
4. The U.S. economy added 57,000 jobs overall in June, with continued gains in professional and business services, social assistance and healthcare.
The post Healthcare job growth slows to 21,500 in June: 4 things to know appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
US death rate drops 4.6%, setting record low: CDC
The nation’s age-adjusted death rate fell 4.6% in 2025 to 689.2 deaths per 100,000 people — the lowest rate ever recorded in the U.S. — according to provisional CDC data published July 2.
An estimated 3,094,593 people died in the U.S. in 2025, according to the report from the CDC’s National Center for Health Statistics, which reflects 99.9% of 2025 death records processed as of May 10. The total number of deaths increased from 3,072,666 in 2024 even as the rate declined.
Five things to know from the report:
1. Death rates fell for every age group and for both sexes. The age-adjusted rate for males (811.1 per 100,000) remained well above the rate for females (582.9).
2. Heart disease remained the leading cause of death with 694,708 deaths, followed by cancer (622,832) and unintentional injuries (184,265). Deaths from heart disease and cancer both increased from 2024.
3. Influenza and pneumonia, recorded together, climbed from the 11th to the 8th leading cause of death, with 56,511 deaths in 2025. The year prior, pneumonia and the flu claimed 48,139 lives. Suicide decreased from the 10th to the 11th leading cause, with 48,789 deaths in 2025.
4. Racial disparities persisted. Age-adjusted death rates were highest for Black Americans (869 per 100,000) and increased for American Indian and Alaska Native people (from 786.1 to 803.8) and Native Hawaiian or other Pacific Islander people (from 682.7 to 746).
The CDC cautioned that rate changes for smaller populations may be skewed by revised census population estimates.
5. The figures are provisional and will likely change as remaining records are processed, particularly unintentional injury deaths, which are reported with a longer lag, meaning the final count will likely be higher. The National Center for Health Statistics typically releases final mortality data about 11 months after the end of each calendar year.
The post US death rate drops 4.6%, setting record low: CDC appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
3 skills new nurses are missing on day 1, per nurse execs
There’s a widening gap between what a nursing degree certifies and what a hospital unit actually demands in practice, nursing leaders say.
New nurses are arriving on the job less prepared for the nuances and complexity of clinical care, leaving hospitals and health systems to increasingly shoulder the additional training and education required for real-world practice.
Many nursing schools are built to produce graduates who pass their licensing exams on the first try, nursing executives told Becker’s, not graduates who are ready for the floor. New data from the National Council of State Boards of Nursing shows registered nurse candidates passed the National Council Licensure Examination-RN exam at a 74.4% rate in the first half of 2026, up from 69.1% in 2025.
Holly Muller, DNP, RN, senior vice president and system chief nursing officer of Presbyterian Healthcare Services in Albuquerque, N.M., has been circling this challenge inside her own system, though she’s not alone.
“I hear this from my peers across the country,” she told Becker’s. “They all have mitigation strategies in place, but what’s happened is, as employers, we’ve had to absorb work that may have — in previous ways in schools — been done to a greater degree than it seems to be done [now].”
Dr. Muller highlighted three specific deficits she sees among new nurses on day one: a lack of critical thinking; compassionate, authentic communication; and basic hands-on experience with clinical procedures.
Several forces are compounding this gap. More low-acuity care has shifted to ambulatory settings over the past 15 years, meaning the patients who remain in acute care are sicker and more medically complex than they were a decade ago. Nursing students who trained during the pandemic, when clinical rotations moved partly or fully virtual, also missed hands-on hours their predecessors had. And the pipeline of experienced nurses available to backfill and mentor is itself shrinking, according to Dr. Muller, since seasoned nurses are largely either settled into roles they do not want to leave or approaching retirement.
The critical thinking skills gap shows up in how new nurses process what is in front of them, according to Donna Berizzi, DNP, RN, associate chief nursing officer of the oncology service line at Johns Hopkins Medicine in Baltimore. The technical pieces, she said, are the easy part to teach. What is harder to teach is synthesizing a patient’s physical, psychosocial and technical needs into a single picture in real time.
“What we can’t teach is how to look at a patient situation and determine all of the things that are going to need to be tied up in a bow all at the same time for them to care for those patients,” Dr. Berizzi said.
The stakes of that gap are high in oncology, where patients can look fine until they suddenly are not, she said. Blood counts can plummet without visible warning signs, and a new nurse may not recognize the pattern quickly enough to escalate in time.
“For a new nurse to be able to understand what that process looks like and being able to escalate in the most complex environment can be incredibly challenging,” she said.
The second gap surfaces in everyday communication between nurses and patients or other members of the healthcare team. When a new nurse calls a physician or an on-call provider to report a concern, Dr. Berizzi said, they often lead with an isolated data point instead of the full clinical picture.
Dr. Muller sees the same erosion from a different angle. Nurses are not just losing comfort with escalation, she said, but the basic skill of connecting with patients and families, in part because of how tethered everyone has become to devices.
“It’s like a lost language,” she said, noting that during her own education, nursing schools had specific modules on team communication.
The third gap is the most literal: hands-on repetition. Dr. Muller said she came through nursing school with more clinical hours than today’s graduates typically get, and could handle most of the clinical assessments her first job required. Today, she said, some new hires have performed a given bedside procedure only once or twice before their first day.
“Nurses are coming out of school with less skills,” she said.
What’s more, the shrinking pool of experienced nurses is straining the system meant to close these gaps. Dr. Berizzi said preceptor pairings do not always work on the first try, and finding a good match takes trial and error. The preceptors who do work well with new hires are asked to carry that load again and again, on top of their own patient assignments.
“A preceptor’s work is doubled when you have them working with a new nurse, and their level of responsibility is doubled,” she said. Demand has outpaced the supply of nurses willing and able to teach. “It’s not fair, it’s not possible,” Dr. Berizzi said.
Health systems are not waiting for nursing schools to close the gap on their own. Presbyterian Healthcare Services opened its Healthcare Advanced Learning Lab, an advanced simulation center, about two years ago and has since made it mandatory for every new nurse. Nurses spend their first week there, working through validated competencies with clinical educators, before ever taking a patient assignment. The system has also built its own framework, called Compassionate Connected Care, to teach caregivers how to interact with patients and their families.
At Johns Hopkins, Dr. Berizzi has moved oncology onboarding away from a fixed timeline entirely. New nurses meet weekly with their preceptor, manager, clinical nurse specialists and educators throughout orientation, and progress through clinical milestones rather than a preset number of weeks before taking on higher-acuity assignments such as chemotherapy administration. Even after formal orientation ends, the transition continues gradually.
“They don’t get a full assignment for weeks,” Dr. Berizzi said.
That oversight extends into daily habits. Dr. Berizzi said her team reviews new nurses’ documentation and checks in with them at the end of every shift.
“We’re reading their notes, we’re meeting with them at the end of the day. How was your day? Tell me a little bit about how you tackle this situation,” Dr. Berizzi said, describing how she makes sure new nurses are seeking out education on their own between shifts.
“A lot of this is like being back in school. They’ve got to go home, they need to read, they need to have access to education,” she said.
For now, Presbyterian and Johns Hopkins — like many other systems — are absorbing this work themselves, one preceptor, one shift and one new nurse at a time.
The post 3 skills new nurses are missing on day 1, per nurse execs appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
When 2 hospitals close: Atlanta’s answer vs. Chicago’s void
Two Chicago-area safety-net hospitals have closed within a year of each other — both owned by Princeton, N.J.-based Resilience Healthcare — and no health system, buyer or partner has publicly committed to reopening either.
Chicago-based Weiss Memorial Hospital, a 239-bed acute care facility, closed Aug. 8, 2025, as CMS moved to terminate its Medicare participation over noncompliance with federal standards for emergency services, nursing services and the physician environment. About 55% of Weiss patients were covered by Medicare and roughly 30% by Medicaid, a payer mix that left too few commercially insured patients to sustain the hospital once Medicare reimbursement ended.
Oak Park, Ill.-based West Suburban Medical Center, Weiss’ sister hospital, closed June 11, after its last working elevator broke down. The hospital on June 30 notified staff of a “mass layoff” effective Aug. 31 that it said is “expected to be permanent,” according to an employee letter obtained by Becker’s.
The closures capped a financial unraveling at Resilience, which acquired the two Chicago hospitals from El Segundo, Calif.-based Pipeline Health System in January 2023.
However, Chicago has absorbed this kind of loss before.
Twenty hospitals in the city closed between 2000 and 2022, nearly 25% of its total, according to Chicago Policy Review. Last year, Ascension St. Elizabeth closed before Ontario, Calif.-based Prime Healthcare acquired it and eight other Illinois hospitals, and Louisville, Ky.-based Kindred closed two Chicago area long-term acute care hospitals.
Atlanta offers a different trajectory.
Atrium Health on June 18 filed a letter of determination to build its first hospital in metro Atlanta, partnering with Morehouse School of Medicine on a short-stay acute care teaching hospital in Fulton County, Ga. The facility would open with 50 beds as the anchor of a 40-acre mixed-use campus.
In public statements, Atrium Health framed the project as a response to closures. The proposed hospital is intended to address care gaps left by two WellStar Health System shutdowns: WellStar AMC South in May 2022 and WellStar Atlanta Medical Center in November 2022. Under the filing, the new hospital cannot exceed 50% of the 762 short-stay beds Atlanta Medical Center held at closure, capping it near 381 beds.
Atlanta-based Grady Health System absorbed the largest influx of patients following the closures and expanded capacity by 180 beds with $130 million in state and federal funding. It also opened neighborhood and specialty clinics. Even so, local leaders have said Atlanta still needs additional hospital capacity to replace the 198-bed AMC South campus and the 460-bed Atlanta Medical Center.
Atrium Health has the scale to make that investment. It is part of Charlotte, N.C.-based Advocate Health, which operates 69 hospitals across six states, and already has a Georgia footprint through Atrium Health Navicent and Atrium Health Floyd.
That scale is also at the heart of Chicago’s challenge.
Rebuilding safety-net capacity in a major urban market requires a well-capitalized operator willing to absorb a Medicare- and Medicaid-heavy payer mix — the same economics that contributed to Weiss’ collapse. No comparable system has signaled interest in Weiss, on Chicago’s North Side, or West Suburban, on the city’s West Side.
However, one major investment is underway elsewhere in the city. Advocate Health Care — also part of Advocate Health — broke ground on a $300 million hospital earlier this month. The 52-bed hospital will replace the current Advocate Trinity Hospital and serve as the centerpiece for the health system’s $1 billion investment in Chicago’s South Side.
For now, pressure to reopen West Suburban is coming from its landlord rather than another health system. Rathnaker Patlola, who owns the hospital’s real estate through Ramco Healthcare Holdings, said the layoff notice violates “the spirit and the letter” of his agreement with Resilience and vowed to take action to ensure the hospital reopens. Manoj Prasad, MD, PhD, Resilience’s CEO, issued the layoff notice.
Becker’s has reached out to West Suburban for comment.
State officials, meanwhile, have underscored the limits of their authority. The Illinois Department of Public Health said the situation was created by a private company, that it received no advance notice of the service suspensions or layoffs, and that it lacks authority over employment decisions, even as it remains “deeply concerned about workforce stability in community hospitals.”
The strategic takeaway for hospital leaders watching from other markets: closures are increasingly clustering at financially fragile safety-net hospitals, and restoring access depends less on regulators than on whether a well-capitalized health system is willing to step in.
Atlanta has a plan to help restore lost capacity. Chicago is still waiting for one.
The post When 2 hospitals close: Atlanta’s answer vs. Chicago’s void appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
The Gen Z, boomer primary care gap: 3 findings
Young adults are far less likely than older generations to maintain an ongoing relationship with a primary care physician, a new survey shows.
The poll was commissioned by Columbus-based OSU Wexner Medical Center and conducted by the survey and market research firm SSRS. The survey includes responses from 1,006 U.S. adults between May 1 and May 3.
Three survey findings:
- Seventy-one percent of adults ages 18-29 reported having a primary care physician, compared with 97% of adults 65 and older.
- Among young adults who do have a primary care physician, just 47% had a checkup in the last year.
- When a nonemergency issue arises, 36% of young adults go to urgent care first, compared with 68% of older adults who contact their primary care physician first.
OSU Wexner noted that primary care is tied to better outcomes, fewer hospital stays and lower emergency department utilization. The findings point to a widening generational divide in care-seeking behavior that health systems will need to address as Gen Z ages into a larger share of the patient population.
The post The Gen Z, boomer primary care gap: 3 findings appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
How 3 hospitals on the brink of closure are fighting to stay open
While 2026 kicked off with fewer hospital closures compared to the same period in 2025, three hospitals in three states are on the verge of closing, and their situations mirror what many facilities across the country are facing.
In Chicago, Roseland Community Hospital has negative 65 days cash on hand, meaning incoming dollars are spoken for before arrival.
Roseland Community made its June 30 payroll because a Medicaid managed care organization made a large volume of claims payments in time to cover it. A $16 million state grant in Illinois’ fiscal year 2027 budget also offers potential relief, but only if the application moves fast.
“When we say that, here’s this grant money that’s there. This stabilizes us,” Tim Egan, president and CEO of Roseland Community Hospital, told Becker’s. “This will help keep the doors open. As I told [Sameer Vohra, MD, director of the Illinois Department of Public Health], who was very compassionate and understands our situation, we’re on our hands and knees begging.”
Roseland Community is also rolling out an austerity plan July 1: a 10% pay cut for senior executives and furloughs for around 30 of the hospital’s roughly 550 employees. Further service line and department cuts are also not being ruled out.
In Montgomery, Ala., Jackson Hospital planned to close by July 1, but pushed the date back as it continues talks with Blue Cross Blue Shield of Alabama, along with city, county and state leaders on a path forward.
Jackson Hospital, which sought bankruptcy protection in February, has been in reimbursement disputes with BCBS Alabama for months.
While the hospital remains operational, CEO John Quinlivan told Becker’s that “important pieces” must be finalized to ensure it remains open.
“I can’t tell you which way it’s going to go, but we are hopeful,” Mr. Quinlivan told Becker’s June 25. “Both organizations want to keep this hospital open. We especially want to keep the hospital open, but we’ve got to have a financial model that makes that possible.”
In Mississippi, financially challenged Greenwood Leflore Hospital saw a small win June 29, after a state Chancery Court judge ordered the state’s Division of Medicaid to release a roughly $2.4 million payment to the hospital.
The payment, expected June 30, aims to keep the hospital open through July 31, when it can be transitioned to a larger system.
On June 18, the Mississippi Institutions of Higher Learning Board of Trustees voted for Jackson-based University of Mississippi Medical Center to take over Greenwood Leflore. The hospital’s property would be donated to UMMC under the approval.
Greenwood Leflore already laid off 86 employees and cut services in April and pushed its closure date back from June 15 to July 31 after a county judge in mid-March temporarily blocked the state Division of Medicaid from collecting a $5.5 million debt from the hospital.
While none of these hospitals have actually closed, each is running on thin ice with outcomes being determined in the days and weeks ahead.
The post How 3 hospitals on the brink of closure are fighting to stay open appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Healthcare burnout looks different now — 5 leaders explain what’s driving it
When the COVID-19 pandemic receded, clinical workers expected three things: sustained recognition for what they had endured, a period of respite and a return to some version of normalcy. Most got none of them.
Instead, they returned to waiting rooms full of patients who had deferred care for years and walked into a new kind of burnout.
“There were a lot of patients waiting to come to the healthcare system,” said David Marcozzi, MD, chief clinical officer of Baltimore-based University of Maryland Medical Center and associate dean of clinical affairs at University of Maryland School of Medicine. “You really weren’t the hero that the public had originally thought you were — and I still consider everyone who came to work a hero. You couldn’t really step away. There was more work to do.”
Years later, the burnout has not disappeared. New AI capabilities have chipped away at documentation burden, but workforce burnout has changed shape, and that shift has made it harder to address.
Five leaders — a chief clinical officer, a chief nurse executive, a chief quality officer and two well-being leaders — described to Becker’s a clinical workforce navigating a new kind of strain: one without a common enemy or a clear end.
From a single cause to many
The defining feature of COVID-19 pandemic-era burnout, several executives said, was that it had a focus. Workers knew what they were battling, and they believed there would be an end.
“In COVID, there was a common cause to save people’s lives, and it was really easy to have that motivation,” said Mary Beth Lardizabal, DO, vice president of mental health and addiction and system medical director of provider well-being at Minneapolis-based Allina Health. “Plus, we had the belief that there would be a cure, there would be an end. Burnout is not like that now.”
What clinicians face today is harder to name. Financial pressure, staffing constraints, regulatory burden, patient volume and institutional uncertainty are all compounding at once.
“There’s stressors coming from so many different angles versus just one,” said Heidi Woodland-Leine, PsyD, manager of provider well-being at Allina Health.
That pressure has specific clinical and legal consequences. When financial constraints force institutions to cut services or change how care is delivered, clinicians experience what Dr. Lardizabal called moral distress — a term she was deliberate about.
“In the COVID pandemic everybody was kind of using all resources available, and now there are less and less resources,” she said. “Clinicians are being asked to do things differently in a way that might not be how they were trained or what they would think is the best possible care, simply because those resources or finances are not available… Some people call it moral injury, but I think the term moral distress captures it.”
Dr. Marcozzi framed the same pressure from a systems perspective. As healthcare expenditures approach 18% to 19% of the nation’s gross domestic product, the burden falls on clinicians: Do more with less.
“The inflection point that healthcare is considering right now is how to work smarter, not harder, with less,” he said.
Burnout looks different by discipline
Documentation burden — which research has consistently linked to physician burnout, including the after-hours charting known as pajama time — has started to ease as ambient AI tools and EHR improvements take hold. But experts caution against seeing AI technology as a general solution.
For nurses, the burnout equation looks different, according to James Ballinghoff, DNP, RN, chief nurse executive at Philadelphia-based Penn Medicine.
“For nursing, I think burnout is more around interactions with people: the disrespect, the violence, the aggression,” Dr. Ballinghoff said. “We spend the majority of time with the patient.”
Staffing is the other major factor, which Dr. Ballinghoff said is not simply nurse-to-patient ratios. When environmental services, food service, phlebotomy or nursing assistant teams run short, registered nurses absorb those gaps.
“Staffing does not necessarily mean RN staffing,” he said, recalling a time when environmental service workers were in short supply, “so there were no linens, [nurses] had to run and get this supply, they had to help turn over a room.”
These additional expectations can weigh on staff.
“The lemon has been squeezed so tight, meaning reimbursements are either flat, sometimes going down, very rarely is it going up, but our expenses went up, our labor costs went up, our supply costs went up, everything went up,” Dr. Ballinghoff said. “It’s just like how we’re living at home, our paychecks can go up, but the price of eggs and gas are going up, and you can’t always rely on your employer to fix that for you.
“We can’t rely on the government paying us the Medicare rates or the payers paying us to cover those increases,” he said. “So, where does it get cut? It gets cut in employees, you know, it always does. And people are feeling that.”
Dr. Ballinghoff also pointed to a subtler structural shift: the design of new hospital buildings. Where nurses once gathered at a central station to document, decompress and build relationships, newer facilities place workstations outside individual rooms, closer to patients, but farther from colleagues.
“Because there’s no longer that nurses station where people would gather and have conversations and create relationships,” he said. “That’s a negative to what you were trying to accomplish as a positive.”
The pizza problem
Organizations trying to address burnout through recognition gestures — catered lunches, T-shirts, Nurses Week giveaways — have found those efforts increasingly counterproductive, executives said, at least in part because of social media.
Dr. Ballinghoff, who monitors nursing influencers with millions of followers to gauge workforce sentiment, described watching content that reframes sincere gestures as insults or shames someone for their profession. At one event, an audience booed a nurse manager after hearing her job title.
“That is the worst message that you can be sending to people: that their managers are out to get them or they’re not supportive,” he said. “When millions of people are hearing that… you can’t underestimate or put your head in the sand that it’s not having an impact in a negative way on our profession.”
The effect is a chilling one: leaders now second-guess gestures they would once have made instinctively.
Dr. Lardizabal was direct about the limits of surface-level interventions: “If that’s your only intervention, you don’t have a well-being program. It has to be much more multifactorial.”
The well-being initiatives most likely to read as empty gestures, she said, are those that cannot be separated from the circumstances that produced them — an organization cutting services, reducing staff or asking clinicians to do more, then offering cold pizza as acknowledgment.
What’s actually working
The institutions seeing the most traction on provider well-being share a few traits: peer infrastructure, compensation for doing well-being work and consistent outcome measurement.
At Allina Health, the center for provider well-being runs refuel groups, direct care psychology and psychiatry services, employee assistance program counseling and a network of well-being leads embedded across the system. Those leads are compensated two hours per week for their well-being work.
“It shows the system that it’s valued,” Dr. Lardizabal said. “[With] the cost of replacing one of those docs, it’s money well spent.”
At NYC Health + Hospitals, Chief Quality Officer and Senior Vice President Hillary Jalon cited the system’s culture of safety infrastructure as the foundation for everything else — including a program called Helping Healers Heal and the reinvigoration of the Just Culture framework in 2024.
The New York City-based system’s most recent employee engagement survey found safety culture scores rising 9% in acute care hospitals and 10% in post-acute care facilities during a period when national scores declined.
“In order for performance improvement to thrive, you need to have a culture of safety,” Ms. Jalon said.
What’s at stake
The stakes of getting this wrong extend well beyond retention figures. A significant share of the clinical workforce is nearing retirement, while the incoming pipeline of physicians and advanced practice providers is smaller and carries different expectations about work and sacrifice.
“Gen Z docs don’t want to do it the way their dads or moms did,” Dr. Lardizabal said. “They really want to have a life, and they’re not going to do the same sacrifice of their health and their time. If you want to recruit those folks, we have to have a different system.”
Dr. Ballinghoff put it plainly: “The joy in work is not there. It’s there in pockets, but it’s not there” the way it was for earlier generations.
Dr. Marcozzi, who was the COVID-19 Incident Commander for the University of Maryland Medical System, framed the moment in terms of what the industry learned from COVID-19 and risks losing.
“We came together and figured it out, and let’s not let those lessons learned fade away,” he said. “We need to accelerate the pace of change and speed of decision, so healthcare can keep up and be ready for the next response.”
The post Healthcare burnout looks different now — 5 leaders explain what’s driving it appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
How a critical access hospital raised its cash on hand from 3 to 25 days
Rawlins, Wyo.-based Memorial Hospital of Carbon County, has grown its days cash on hand from 3 days to 25 days between January 2025 and June 2026, marking a significant financial recovery for the 25-bed critical access hospital.
The turnaround also includes a reduction in outstanding payables from more than $9 million to under $3 million, according to a June 24 news release from the hospital. Memorial’s leadership also established a dedicated reserve fund to protect payroll during periods of financial stress.
“These improvements didn’t happen overnight,” CEO Kerry Ashment said in the release. “They are the result of thoughtful planning, accountability, and a shared commitment to securing the hospital’s future.”
Revenue cycle improvements were a key part of the hospital’s financial recovery. Memorial brought medical coding in-house, partnered with a new revenue cycle management firm, streamlined payer enrollment and strengthened payer relationships. These efforts have helped better position the hospital to capture revenue appropriately while reducing administrative delays and inefficiencies.
The hospital also conducted a compensation analysis in early 2026 and adjusted wages for several positions to improve recruitment and retention competitiveness.
Leadership has adopted a three-year strategic plan that outlines priorities for financial sustainability, service delivery and community engagement. Memorial has also adopted Lean business principles across departments, with managers receiving ongoing education and support to identify waste, improve processes and enhance overall performance.
Hospital leaders said that while meaningful progress has been made, the work is ongoing and Memorial will continue to focus on financial stewardship, operational efficiency and workforce development.
The post How a critical access hospital raised its cash on hand from 3 to 25 days appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
How marketing is becoming a health system growth engine
Health system chief marketing officers say marketing is most effective when it helps shape strategy instead of simply promoting it.
As executives face growing pressure to demonstrate measurable business results, Becker’s asked marketing leaders to share a campaign or initiative that moved the needle on revenue and what it revealed about marketing’s role in driving organizational growth.
At UW Medicine in Seattle, the proof of concept came from an access problem. Patients seeking evaluation for complex neurological conditions, including brain aneurysms, moyamoya disease, meningiomas, cavernomas and arteriovenous malformations, often faced friction that had nothing to do with clinical capacity. Getting to a neurosurgical consultation meant navigating traditional referral processes or waiting in call center queues.
A neuroscience marketing manager developed a digital self-referral pathway: condition-specific online appointment forms that allowed patients to request a neurosurgical consultation at any time and have submissions routed directly to the scheduling team. Within the first year, one pathway generated 44 completed neurosurgical consultations and 18 completed neurosurgeries, a 41% surgical conversion rate from completed appointments.
“Marketing is most effective when viewed not simply as a communications function, but as a strategic growth partner that helps remove barriers to care, improve the patient experience and create measurable pathways from awareness to treatment,” said Glenn Bieler, chief brand and marketing officer at UW Medicine, along with senior marketing manager Jamie Kahn and assistant director of marketing Jenny Ring-Perez. “When marketing is empowered to solve access challenges and collaborate closely with clinical and operational teams, it can deliver meaningful outcomes for patients, clinicians and the organization alike.”
At Coral Gables, Fla.-based Baptist Health South Florida, marketing’s role in growing the health system’s urgent care service line began well before anyone wrote a creative brief. Baptist Health has operated urgent care sites in South Florida for nearly 30 years, but a more competitive same-day care market demanded a rethinking of the service itself.
Christine Kotler, chief marketing and communications officer, said the marketing team entered the process at the strategy level, defining the business challenge, convening cross-functional stakeholders and leading consumer research before any campaign work began. Ethnographic research revealed that convenience and speed had become table stakes. What actually drove choice and loyalty was the total experience: the physical environment, the emotional tone and the ease of access.
One of the most consequential findings was that patients did not separate the quality of care from the quality of the environment. They expected urgent care spaces to feel modern, clean and welcoming, closer to hospitality than a traditional clinical setting.
Marketing translated those insights into facility redesigns, upgraded materials, more intuitive layouts and staff training before developing a single piece of advertising. The campaign that followed, “The Better Way to Better,” used a “green carpet” as a signature creative device to signal an elevated, differentiated experience, positioning Baptist Health above transactional retail care options on trust, warmth and quality rather than speed alone. Same-day care volumes have increased 8.21% year over year, with off-campus emergency department volumes growing 39.37%.
“When positioned upstream and empowered to influence the business before campaign development begins, marketing can help define not only how a service is communicated, but how it is experienced, differentiated and grown,” Ms. Kotler said. “Our brand is not defined by the advertising, but rather by the complete experience.”
At Mountain View, Calif.-based El Camino Health, Mark Klein, chief communications and marketing officer, described a deliberate move away from a communications-and-campaign model toward what he calls an enterprise growth capability that integrates brand strategy, precision marketing, consumer data and measurable patient acquisition.
Over a six-month period, the team deployed targeted growth campaigns across nine strategic service lines, including primary care and urgent care, generating more than 7,000 new patients and more than 70,000 verified visits. The campaigns produced more than $16 in attributable revenue for every dollar invested. Over the same period, unaided brand awareness increased by nearly 60%.
“The most important shift is moving from ‘marketing as expense’ to ‘marketing as a disciplined investment in growth,’” Mr. Klein said. “That reframing changes how we resource the function, how we measure success and how leadership engages with marketing as a strategic partner rather than a support function.”
At Marlton, N.J.-based Virtua Health, Chief Marketing Officer Chrisie Scott said the team built a shared ROI framework with finance that it regularly presents to leadership and the board. The work spans CRM-powered campaigns that bring patients back for critical screenings, including mammograms and colonoscopies, to propensity models that connect patients to specialized care.
Ms. Scott singled out a less data-driven initiative as one of the most instructive: a series of live virtual “real talk” women’s health chats in which physicians discuss topics from mental health to sexual wellness without a script. The format has consistently attracted both new patients and more engaged existing ones.
“It’s a powerful reminder of the impact marketing has when we allow our consumers’ voice to guide our approach,” Ms. Scott said. “In healthcare, where every operational dollar is vital, marketing must be able to connect what we do to quantifiable brand, business and human outcomes.”
The post How marketing is becoming a health system growth engine appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Hiring, pay and restructuring: 4 HR leaders on difficult workforce decisions
From restructuring leadership teams to limiting hiring and adjusting compensation, health system leaders are making difficult workforce decisions that require balancing organizational priorities, financial realities and employee needs.
While the circumstances vary, those decisions often require balancing several competing priorities at once. Becker’s asked three health system leaders: What is the hardest workforce decision you’ve made in the past year, and what did it teach you?
Editor’s note: Responses are lightly edited for length and clarity.
Amy Beales. Chief Human Resources Officer for Luminis Health (Annapolis, Md.): The hardest workforce decisions are often the ones that ask people to let go of what has always been in order to build what comes next. During periods of organizational transformation here at Luminis Health, we are trying to standardize practices, redesign leadership structures and create one culture for many. Those decisions aren’t always easy, but they reinforce that successful change depends less on the decision itself and more on how leaders communicate, listen, and bring people along as we strive to be a truly great workplace.
Wendy Fournet, EdD. Executive Vice President and Chief Administrative Officer for Erlanger (Chattanooga, Tenn.): One of the hardest workforce decisions I made in the past year was implementing a more disciplined workforce management process (i.e. a labor council) during a period of significant financial and operational pressure. As part of that effort, we required executive-level review and approval for new positions and backfills across the organization, while balancing the needs of an academic health system with 8,000 employees and the reality of workforce shortages in healthcare.
The challenge was that every leader could make a compelling case for why their position was critical. Patient care, employee well-being, physician support and financial stewardship were all competing priorities. There were times when we had to delay or reconsider positions that departments genuinely needed, even though we understood the operational impact.
What made the decision difficult was recognizing that workforce decisions are not simply about headcount — they are about people, workload, patient access and organizational sustainability. Saying “not now” to a position often meant asking leaders and teams to continue carrying additional responsibilities in the short term.
The experience taught me three important lessons:
- Transparency matters. Leaders are much more likely to support difficult workforce decisions when they understand the criteria, the data and the broader organizational context behind them.
- Workforce planning must be strategic, not reactive. Every position should be evaluated based on its contribution to patient care, growth, operational efficiency and long-term organizational goals rather than historical staffing models.
- People and finances are not competing priorities. Sustainable financial stewardship ultimately protects jobs, allows us to invest in our workforce and ensures we can continue fulfilling our mission for years to come.
While those conversations were difficult, the process strengthened our leadership team’s ability to think strategically about talent and resources. It reinforced that some of the most important workforce decisions are not about adding positions, but about ensuring we are building an organization that can continue to support our employees, physicians and patients well into the future.
Stacey Hancock. Senior Vice President and Chief Human Resources Officer at Archbold (Thomasville, Ga.): The hardest workforce decision I’ve made in the past year was implementing market-based pay adjustments across our system while ensuring internal equity and long-term financial sustainability.
Like many health systems, we were facing significant external pressure on wages — particularly in nursing and other high-demand roles. The data clearly showed we needed to act to remain competitive and retain talent. However, making targeted adjustments introduced real challenges around compression, equity between tenured and newly hired team members, and the broader impact on our overall compensation structure.
The difficult part of this decision wasn’t recognizing the need — it was determining how to do it responsibly. We had to make thoughtful choices about where to prioritize investments, how to communicate transparently with leaders and team members and how to manage expectations when we couldn’t address every concern at once.
What this taught me is that workforce decisions at this level require both discipline and empathy. You have to be grounded in data and strategy, but equally committed to fairness, consistency and clear communication. It also reinforced that there is rarely a perfect solution — only the most responsible one given your mission, your resources and your people.
Ultimately, it strengthened our approach to compensation governance and reinforced the importance of taking a long-term, systemwide view rather than reacting to short-term pressures.
Joline Treanor. System Chief Human Resources Officer at City of Hope (Duarte, Calif.): One of the most complex workforce challenges this past year was helping lead through a period of significant organizational change while balancing the needs of our people, patients and long-term strategic priorities. For a CHRO, moments like these reinforce the importance of clear communication, transparency and consistency, especially when teams are navigating uncertainty.
Most importantly, they are a reminder that every workforce decision affects real people and families. As leaders, we have a responsibility to approach these moments with thoughtfulness and intention, helping individuals navigate what is ahead while keeping teams moving forward with clarity and confidence, guided our values of inclusion, integrity and compassion.
The post Hiring, pay and restructuring: 4 HR leaders on difficult workforce decisions appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Hospitals cite technical issues for price transparency notices
Many of the 519 hospitals that drew federal price transparency warning letters from the Trump administration said the citations stemmed from minor technical or formatting errors in their data files — not a failure to disclose pricing — and that the problems were corrected within days of notification.
The Associated Press exclusively received a list of hospitals that have either received warning letters or requests to submit plans to provide transparency pricing since April. A senior administration official who requested anonymity told the news outlet that President Donald Trump plans to ramp up price transparency enforcement and more hospitals are likely to receive letters for failure to comply.
Becker’s spoke with more than a dozen health systems with hospitals that were among the 519 that received notice letters. The systems said their issues were tied to technical or formatting issues rather than missing pricing data.
Among them was Pittsburgh-based Allegheny Health Network, whose flagship academic medical center, Allegheny General Hospital, received a warning notice from CMS. An Allegheny Health Network spokesperson told Becker’s the hospital received the notice in April and the issue raised by the administration was “rectified immediately.”
“Importantly, the only issue raised by CMS was not a transparency issue, it was a small technical/clerical issue,” the spokesperson said. “We submitted a file that included our DBA name (Allegheny General Hospital) but did not include our legal entity name (West Penn Allegheny Health System).”
Allegheny Health Network received written confirmation in May that CMS was satisfied with the fix and the issue is now closed.
Greenville, N.C.-based ECU Health received warning notices at two of its hospitals, its flagship ECU Health Medical Center and ECU Health Beaufort Hospital in Washington, N.C.
An ECU Health spokesperson said that for its flagship hospital, CMS identified technical issues with the machine-readable file that affected compliance with certain formatting requirements, and the identified technical issues were corrected within the timeframe allowed by CMS.
The notice received by ECU Health Beaufort Hospital involved a separate issue related to its organizational structure. The hospital is a campus of ECU Health Medical Center. Pricing information was already publicly available as part of the flagship hospital’s file.
“We have since taken additional steps to post a separate machine-readable file for the Beaufort campus to further facilitate patient access to pricing information specific to that location,” the ECU Health spokesperson said.
Jeremy Farnum, director of information services at Lompoc (Calif) Valley Medical Center said CMS identified three encoding errors in the hospital’s machine-readable file. He said the issues did not involve missing pricing data or an unwillingness to disclose charges. There were formation issues in how the data was structured within the MRF.
“Upon receiving the notice, we worked with our MRF hosting vendor to identify and correct all three errors,” Mr. Farnum said. “We also prepared a corrective action plan to formalize the fixes and prevent recurrence. We support the goals of price transparency and have been committed to compliance since the rule took effect. The increased enforcement focus reinforces the importance of the technical precision required in MRF files, and we’ve tightened our internal review processes accordingly.”
New price transparency rules took effect for hospitals April 1 covering machine-readable files, with changes focused on attestation language and executive accountability for file accuracy, percentile allowed amount reporting, and National Provider Identifier reporting. Multiple health systems noted the new rules in their responses to Becker’s, including King of Prussia, Pa.-based Universal Health System, which had several facilities receive notices from CMS following the updated requirements.
“The primary issue that has been raised was a technical one dealing with the manner in which our facilities were identified and not one related to the disclosure of pricing information,” a UHS spokesperson said. “All pricing information was provided. Upon notification, we reviewed the matter and facilities have implemented the necessary corrections. Most facilities have since received notice of resolution from CMS.”
Federal price transparency laws have been in effect for hospitals since Jan. 1, 2021, and July 1, 2022, for payers. CMS has fined 28 hospitals for alleged price transparency violations since the law took effect in 2021. Ten hospitals were fined in 2025, and one hospital has been fined so far in 2026.
The post Hospitals cite technical issues for price transparency notices appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
8 GLP-1 findings to know
A wave of new research is expanding what clinicians and health system leaders know about GLP-1 medications — covering new territory from liver disease to male fertility to a blood pressure safety signal.
Here are eight recent findings:
- GLP-1 medications did not harm male hormones or fertility after long-term use and may improve testosterone and sperm quality in men with obesity-related low testosterone. Researchers said the findings support treating underlying obesity as a driver of low testosterone rather than defaulting to testosterone replacement therapy.
- Researchers at Chicago-based Northwestern Medicine identified a hypotension safety signal in GLP-1 users already taking multiple blood pressure medications, according to a June 13 system news release. In an analysis of more than 42,000 adults, hypotensive events — including dizziness, fainting and falls — rose from 8.7% to 10.2% within six months of starting GLP-1 therapy, with risk remaining elevated at 12 months. Adults 65 and older accounted for 53% of events despite representing 37% of the study population. Researchers said weight loss alone did not explain the increased risk and urged clinicians to monitor high-risk patients, particularly those obtaining GLP-1s without physician oversight.
- Middle-age adults using GLP-1s for obesity could save an average of $192,735 in lifetime medical costs. Adults starting treatment between ages 25 and 30 could save as much as $270,800.
- Drugmakers including Pfizer, Roche, Boehringer Ingelheim and Amgen are developing next-generation GLP-1 therapies targeting injection frequency, gastrointestinal side effects and muscle mass loss. Boehringer Ingelheim reported Phase 3 data showing its GLP-1 and glucagon combination reduced lean-mass loss to 10.8% of total weight lost — versus 25% to 40% with current therapies — while delivering 16.6% average total body weight loss over 72 weeks. Pfizer is testing a monthly formulation that could cut injections from 52 per year to as few as 13.
- Eli Lilly’s oral GLP-1 Foundayo (orforglipron) outperformed oral semaglutide on blood sugar control and weight loss in the first head-to-head Phase 3 trial of two oral GLP-1 therapies. At 52 weeks, patients on Foundayo 17.2 milligrams lost 19.7 pounds on average, versus 11 pounds for oral semaglutide.
- An experimental dual agonist, survodutide, produced significant liver fat reduction and weight loss in a Phase 3 trial of adults with metabolic dysfunction-associated steatotic liver disease, according to a study conducted by researchers in the U.S., Candada and Europe and published June 7 in Nature Medicine. Among patients given survodutide over 48 weeks, 84% reduced liver fat by at least 30% versus 24% on placebo, and 61% reached normal liver fat levels versus 5.7% on placebo. Patients also lost an average of 12% of body weight versus 1% on placebo. The drug has received FDA Breakthrough Therapy Designation.
- GLP-1 use was linked to lower incidence and improved outcomes across multiple cancer types, including breast, colorectal, prostate, pancreatic, liver and non-small cell lung cancers. Among more than 841,000 breast cancer patients, GLP-1 use was associated with reduced all-cause mortality and lower recurrence risk in patients with obesity or Type 2 diabetes.
- Oral Wegovy surpassed 3 million prescriptions in just over five months following its Jan. 5 U.S. launch — roughly one script every five seconds. The milestone comes as the oral GLP-1 market intensifies, with Lilly’s June head-to-head data directly contesting Novo’s earlier claims that oral semaglutide outperforms orforglipron on weight loss and GI tolerability.
The post 8 GLP-1 findings to know appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
How 25 health systems’ labor costs trended in Q1
Workforce spending remained hospitals’ top expense in 2025, representing 60% of total expenses, according to the American Hospital Association.
Workforce costs rose 5.6% in 2025 as hospitals continued increasing wages and investing in recruitment and retention efforts for nurses, physicians and other staff, according to the AHA’s 2026 “Cost of Caring” report.
First-quarter financial reports show those workforce investments continued into 2026, with labor costs rising across most health systems. Here is how 25 health systems’ labor costs changed year over year during the three months ended March 31:
Adventist Health (Roseville, Calif.)
Employee compensation: $879 million (+1.3% YOY)
Advocate Health (Charlotte, N.C.)
Salaries, wages and benefits: $5.5 billion (+8.1% YOY)
Banner Health (Phoenix)
Salaries, benefits and contract labor: $1.8 billion (+5.9% YOY)
BayCare Health System (Clearwater, Fla.)
Salaries and benefits: $708.5 million (+6.4% YOY)
BJC Health System (St. Louis)
Salaries and benefits: $1.5 billion (+8.2% YOY)
Bon Secours Mercy Health (Cincinnati)
Employee compensation: $1.7 billion (+4.1% YOY)
Cleveland Clinic
Salaries, wages and benefits: $2.5 billion (+5.1% YOY)
Corewell Health (Southfield, Mich.)
Salaries, wages and employee benefits: $1.6 billion (+3.6% YOY)
HCA Healthcare (Nashville, Tenn.)
Salaries and benefits: $8.3 billion (+3.6% YOY)
Indiana University Health (Indianapolis)
Salaries, wages and benefits: $1.3 billion (+3.6% YOY)
Inova Health System (Falls Church, Va.)
Salaries and benefits: $955.2 million (+6.6% YOY)
Intermountain Health (Salt Lake City)
Employee compensation and benefits: $2 billion (+5.1% YOY)
Kaiser Permanente (Oakland, Calif.)
Salaries, wages and benefits: $7.4 billion (+3% YOY)
Mayo Clinic (Rochester, Minn.)
Salaries and benefits: $2.8 billion (+5.8% YOY)
Montefiore Health System (New York City)
Salaries, wages and employee benefits: $1 billion (+1.5% YOY)
Mount Sinai Health System (New York City)
Salaries, wages and benefits: $1.5 billion (-3.3% YOY)
Novant Health (Winston-Salem, N.C.)
Salaries and employee benefits: $1.5 billion (+12.9% YOY)
Presbyterian Healthcare Services (Albuquerque, N.M.)
Salaries, wages and employee benefits: $454.2 million (+9.6% YOY)
Providence (Renton, Wash.)
Salaries and benefits: $4.1 billion (+6.6% YOY)
Renown Health (Reno, Nev.)
Salaries, wages and employee benefits: $226.7 million (+4.4% YOY)
SSM Health (St. Louis)
Salaries and benefits: $3.3 billion (+12.8% YOY)
Sutter Health (Sacramento, Calif.)
Salaries and employee benefits: $2.3 billion (+6.9% YOY)
Texas Health Resources (Arlington)
Salaries, wages and employee benefits: $996.3 million (+12.8% YOY)
University Hospitals (Cleveland)
Salaries, wages and employee benefits: $965.9 million (+5.5% YOY)
UPMC (Pittsburgh)
Salaries, professional fees and employee benefits: $2.7 billion (+4.9% YOY)
The post How 25 health systems’ labor costs trended in Q1 appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Rural physicians are leaving Medicare faster than anyone is tracking
Nationally, roughly 1% of U.S. physicians have opted out of Medicare entirely, according to 2025 data from KFF.
While 1% appears to be a marginal number upon first glance, a closer look at where those exits are happening, and what is accelerating the trend, tells a more consequential story for independent physician practices and the ASCs that depend on them.
A 2025 JAMA analysis of Medicare claims data from 2013 to 2023 found that while overall physician participation in Medicare grew by 6.3% over that decade, physicians in nonmetropolitan counties were more likely to exit the program than their metropolitan counterparts.
Physicians practicing in Health Professional Shortage Areas — communities already struggling to maintain adequate care capacity — were also disproportionately leaving.
Notably, female physicians exited at a rate of 3.16%, compared with 2.39% for male physicians, a disparity the study’s author, Christopher Whaley, PhD, of Brown University in Providence, R.I., linked in part to the fact that female physicians are overrepresented in primary care, where Medicare reimbursement pressure has been most acute.
The financial logic driving those exits has been building for decades. According to the American Medical Association, Medicare reimbursement for physician services has declined 33% from 2001 to 2026 when adjusted for inflation, with some fee schedule provisions unchanged since 1992.
“Unfortunately, physicians are losing money in multiple scenarios in medicine,” Taif Mukhdomi, MD, interventional pain physician at Columbus, Ohio-based Pain Zero, told Becker’s in 2025. “The most prominent loss of physician revenue is Medicare’s consistent decreasing of physician reimbursement in office settings while supporting hospital-setting healthcare services. This trend affects all insurances, as Medicare is the benchmark of most if not all healthcare insurance reimbursement.”
The compounding effect of that benchmark problem is what makes individual opt-out decisions a systemic indicator rather than an isolated one. When Medicare cuts, commercial payers often follow — making the economic calculus for staying in the program worse with each rate cycle.
The opt-out rate and practice closure rate are distinct metrics, but they trace the same root cause. Becker’s reported 23 physician practice closures in 2025, with continued closures into 2026 — including the shuttering of four primary care clinics by Johnson City, Tenn.-based State of Franklin Healthcare Associates in January.
Whether a physician opts out of Medicare or closes a practice entirely, the downstream effect on patient access is similar, and the entity stepping into that gap increasingly is not another independent physician.
Payer-operated practices now account for 4.2% of the national Medicare primary care market by service volume, up from just 0.8% in 2016, according to a July 2025 study in Health Affairs Scholar. In counties with above-average Medicare Advantage enrollment, that share rises to 5.5%. Independent physicians exiting Medicare are increasingly being replaced by vertically integrated entities.
For ASCs, that consolidation dynamic carries real operational stakes. ASC volume is largely physician-driven: independent surgical specialists who control their own referral patterns are the partner base that sustains most physician-owned centers. As those physicians face escalating pressure — rate cuts, administrative burden, rising practice costs — the population of potential ASC partners is narrowing, and the alternatives available to them increasingly point away from the independent practice model entirely.
The 2026 Hospital Outpatient Prospective Payment System final rule moved Medicare further toward equalizing rates across sites of care, added 560 codes to the ASC covered procedures list and phased out 285 primarily musculoskeletal procedures from the inpatient-only list. CMS estimated the changes would reduce OPPS spending by roughly $290 million in 2026. For independent physician groups, site neutrality levels the playing field between their practice and larger, vertically integrated systems and hospitals, while also removing the reimbursement penalty for directing surgical cases to ASCs rather than HOPDs.
“If reimbursement suddenly shifted to site-neutral payments, private practices would immediately redirect as many appropriate cases as possible from hospitals to their own ASCs, since the financial disadvantage of performing cases outside the hospital would disappear overnight,” Brian Curtin, MD, an orthopedic surgeon at OrthoCarolina Hip and Knee Center in Charlotte, N.C., told Becker’s.
In terms of legislative reform, a bipartisan group of lawmakers in March introduced the Provider Reimbursement Stability Act, led by Rep. Greg Murphy, MD, a Republican from North carolina. The bill would raise the budget neutrality threshold from $20 million to $54.3 million, index it to inflation every five years, limit year-to-year conversion factor variance to 2.5% and require updates to practice expense calculations at least every five years. If enacted, the bill would represent the most structural fix to physician fee schedule mechanics since MACRA.
The post Rural physicians are leaving Medicare faster than anyone is tracking appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
As the nursing landscape evolves, the art of caring remains critical
My mom was a nurse. Some of my most vivid childhood memories are of accompanying her on house calls, where she taught husbands and wives how to give insulin injections using an orange for practice. Growing up in Bayonne, N.J., my mother was the trusted soul of our community and the person everyone turned to when they had a problem. Watching her care for others, I knew I wanted to dedicate my life caring for people, too.
Nearly four decades later, healthcare looks very different. At Hackensack Meridian Health, a virtual nurse can support a bedside team from a remote workstation. Generative AI can help draft our nursing notes. And care can now be delivered directly in patients’ homes. The tools have changed in ways my mother would hardly recognize, but the heart of the work has not. The trusted soul at the bedside is still the same job she did at our kitchen table in Bayonne.
How health leaders choose to integrate technology will determine whether the next generation of nurses can maintain the art of caring. Too much of the conversation around AI in healthcare is framed in terms of productivity and cost savings. That mindset will drive nurses away. If health systems use AI primarily to cut labor costs instead of enhancing humanity in care delivery, we will only accelerate the burnout crisis we are trying to solve.
The better approach is to see technology as a way to create more time for patient connection, not less. Every AI tool and new virtual platform is only worth deploying if it gives bedside nurses more capacity to build meaningful connections with patients.
At HMH, our philosophy is not built around maintaining the status quo. We are not comfortable with mediocrity, and we are not interested in simply getting by. We believe the only way to redefine health care and improve outcomes for our patients is to innovate aggressively. But our approach to innovation is deliberate; we are deploying technology precisely where administrative burdens pull our nurses away from their patients.
Virtual nursing is one of the strongest examples of that philosophy in practice. We launched the program two years ago, and today we have 147 integrated beds across four hospitals where remote team members tag-team with bedside nurses on admission, discharge, education and documentation. With the help of the virtual team, the bedside nurse can spend more meaningful time with patients.
We are also using Epic’s generative AI to assist with nursing documentation, and our Hospital from Home program has cared for more than 2,000 patients since January 2024. Together, these innovations have helped expand nursing capacity, while safeguarding the human connection that must be at the center of care.
Amid a national nursing shortage and a burnout crisis, HMH’s 2025 nurse vacancy rate is 4.5%, compared with the national average of 9.6%. This result only happens when you deploy technology to protect the time nurses spend connecting with and caring for patients.
The human connection and the complex, real-time decision-making that happens at the bedside cannot be replaced by technology. The art of caring — empathy, compassion and an unwavering commitment to improving the patient experience — is what truly reaches patients in their most vulnerable moments. It is what our 9,000 nurses bring to every shift and every patient interaction. And it is something no chatbot or virtual platform will ever replace.
I encourage health system leaders to ask a simple question when evaluating new technology: Will this give our nurses more time to be human with patients, or will it pull them away from the bedside? Investments that pass that test will strengthen our workforce, improve outcomes and build more resilient systems of care.
For nurse leaders and aspiring nurses entering the profession, the message is equally important. Embrace the change. The tools will keep evolving. But the art of caring is ours to protect.
I draw on my nursing foundation every single day. Although I am no longer at the bedside, I am alongside our nurses at one of our sites weekly, because nursing is in my DNA. My “why” began at a kitchen table in Bayonne and it has never left me.
What happens within the four walls of our hospitals is only a small part of a patient’s story. We are committed to caring for our patients for the rest of their lives. The tools may continue to evolve, but every patient still needs what my mother gave her neighbors: trust, compassion and a nurse who knows how to care.
The post As the nursing landscape evolves, the art of caring remains critical appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Top universities for radiology, nuclear medicine: US News
Cambridge, Mass.-based Harvard University was ranked the top university for radiology, nuclear medicine and medical imaging — both globally and in the U.S. — as part of U.S. News & World Report’s “2026-2027 Best Global Universities” rankings.
Harvard University also earned the top spot for overall best global university, according to a June 16 news release from U.S. News & World Report.
U.S. News ranked more than 2,250 universities overall and by 51 subject areas based on data collected by Clarivate from 2020 to 2024. Read more about the methodology here.
Here are the top 25 U.S. universities for radiology, nuclear medicine and medical imaging according to U.S. News, listed with subject score:
1. Harvard University (Cambridge, Mass.): 100
2. Stanford (Calif.) University: 87
3. Johns Hopkins University (Baltimore): 83.9
4. University of Pennsylvania (Philadelphia): 82.2
5. University of California San Francisco: 81
6. Icahn School of Medicine at Mount Sinai (New York City): 76.1
7. University of California Los Angeles: 76
8. University of Michigan Ann Arbor: 74.7
9. Cornell University (Ithaca, N.Y.): 73.7
10. University of Wisconsin Madison: 72.2
11. Yale University (New Haven, Conn.): 72
12. Duke University (Durham, N.C.): 71.3
13. New York University (New York City): 68.3
14. Emory University (Atlanta): 66.5
15. Massachusetts Institute of Technology (Cambridge, Mass.): 66.4
16. University of North Carolina (Chapel Hill): 66.2
17. Washington University in St. Louis: 65.5
18. University of Washington (Seattle): 65.1
19. University of Texas Southwestern Medical Center (Dallas): 64.6
20 (tied). University of California San Diego: 63.4
20 (tied). University of Southern California (Los Angeles): 63.4
22. University of Pittsburgh: 61.9
23. University of Maryland Baltimore: 61.5
24. Vanderbilt University (Nashville): 59.1
25. Columbia University (New York City): 58.9
Read the full ranking here.
The post Top universities for radiology, nuclear medicine: US News appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Georgia health system names director of nursing
Valdosta, Ga.-based SGMC Health has appointed Sarah Durden, BSN, RN, as director of nursing for acute care.
In the role, Ms. Durden oversees nursing operations across 3 West, 4 South and virtual nursing program, according to a June 15 hospital news release.
Ms. Durden brings more than 16 years of nursing experience to the position. She began her healthcare career in the emergency department as a unit clerk and patient care technician before becoming a registered nurse and serving on a medical-surgical unit.
She has since served in clinical supervisory roles in extended recovery and as a nurse manager, according to the release.
The post Georgia health system names director of nursing appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Virtual nursing tied to 72% drop in ED readmissions: 9-hospital study
Virtual nursing for hospital discharge was associated with sharply lower 30-day emergency department readmissions across nine hospitals in a major Southeastern U.S. health system, according to a study published in npj Digital Medicine.
Researchers at the University of North Carolina at Chapel Hill compared 4,662 discharges handled by remotely located virtual nurses with 4,662 traditional in-person discharges, matched on patient and hospital characteristics. Patients discharged through virtual nursing returned to the ED within 30 days at a rate of 3.7%, versus 13.3% for in-person discharge — a 72% relative reduction, or a risk ratio of 0.28. That works out to roughly 1 readmission in 27 virtual-nursing patients, compared with 1 in 8 receiving standard discharge.
The effect held in both settings, with the gap widest in rural hospitals: 3.1% versus 17.9% rural, and 4.1% versus 10.7% urban.
Virtual nurses delivered structured, uninterrupted discharge education — medication reconciliation, teach-back, and care-plan review — from an off-site center operating 7 a.m. to 7 p.m., seven days a week. The health system rolled out the model across the nine hospitals between 2022 and 2024.
The study was retrospective and observational, so it shows association rather than causation; the authors flagged possible residual confounding and a single-system scope, and called for randomized trials and cost-effectiveness research.
For hospital leaders weighing virtual nursing amid persistent staffing shortages, the findings offer some of the first multisite, patient-outcome evidence that the model can streamline discharge without compromising short-term safety.
The post Virtual nursing tied to 72% drop in ED readmissions: 9-hospital study appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
100 hospital financial benchmarks | 2026
S&P Global Ratings’ preliminary 2025 medians show nonprofit hospitals and health systems posting positive but still-thin operating margins, stronger debt-service coverage and growing reserves, with performance varying across credit tiers. Hospitals enter the back half of 2026 managing elevated labor and drug costs, an eroding payer mix and the looming reimbursement changes of HR 1.
Below are 100 hospital financial benchmarks from the most recent reports available from S&P Global Ratings, Moody’s Ratings, Kaufman Hall and KFF:
S&P Global Ratings preliminary 2025 medians
Source: S&P Global Ratings, “Preliminary 2025 Medians For U.S. Not-For-Profit Acute Health Care Providers Indicate Incremental Improvement,” published May 7, 2026, based on 238 audits. Final medians on roughly 400 rated entities are due in the third quarter of 2026.
All acute care providers (standalone hospitals and systems combined)
- Median operating margin: 1.2%
- Excess margin: 4.3%
- Operating EBIDA margin: 6.2%
- EBIDA margin: 8.9%
- Maximum annual debt service coverage: 4.4x
- Operating lease-adjusted coverage: 3.8x
- Unrestricted days’ cash on hand: 208.2
- Unrestricted reserves to total long-term debt: 204.8%
- Capital expenditures to depreciation: 133.6%
- Long-term debt to capitalization: 26.3%
- Median total operating revenue: $2.18 billion
Health systems
- Median operating margin: 1.5%
- Excess margin: 4.1%
- Operating EBIDA margin: 6.0%
- EBIDA margin: 8.2%
- Maximum annual debt service coverage: 4.8x
- Operating lease-adjusted coverage: 3.6x
- Unrestricted days’ cash on hand: 207.6
- Unrestricted reserves to total long-term debt: 207.7%
- Capital expenditures to depreciation: 145.1%
- Long-term debt to capitalization: 26.5%
Standalone hospitals
- Median operating margin: 1.1%
- Excess margin: 4.8%
- Operating EBIDA margin: 6.3%
- EBIDA margin: 9.8%
- Maximum annual debt service coverage: 4.2x
- Operating lease-adjusted coverage: 3.9x
- Unrestricted days’ cash on hand: 210.6
- Unrestricted reserves to total long-term debt: 200.2%
- Capital expenditures to depreciation: 102.8%
- Long-term debt to capitalization: 25.7%
“AA” rating category
- Median operating margin: 3.4%
- Excess margin: 8.1%
- EBIDA margin: 12.4%
- Maximum annual debt service coverage: 7.9x
- Unrestricted days’ cash on hand: 309.0
- Unrestricted reserves to total long-term debt: 327.8%
- Capital expenditures to depreciation: 172.9%
- Long-term debt to capitalization: 17.7%
“A” rating category
- Median operating margin: 1.5%
- Excess margin: 4.3%
- Operating EBIDA margin: 6.2%
- EBIDA margin: 8.8%
- Maximum annual debt service coverage: 4.4x
- Unrestricted days’ cash on hand: 207.7
- Unrestricted reserves to total long-term debt: 196.7%
- Capital expenditures to depreciation: 138.3%
- Long-term debt to capitalization: 27.5%
“BBB” rating category
- Median operating margin: -0.1%
- Excess margin: 1.2%
- Operating EBIDA margin: 3.9%
- EBIDA margin: 6.0%
- Maximum annual debt service coverage: 2.8x
- Operating lease-adjusted coverage: 2.4x
- Unrestricted days’ cash on hand: 113.2
- Long-term debt to capitalization: 34.9%
Speculative-grade
- Median operating margin: -1.0%
- Excess margin: 0.0%
- Operating EBIDA margin: 3.8%
- EBIDA margin: 4.7%
- Maximum annual debt service coverage: 1.9x
- Operating lease-adjusted coverage: 1.7x
- Unrestricted days’ cash on hand: 67.0
- Long-term debt to capitalization: 50.2%
Payer mix, volume and growth
Source: Moody’s Ratings nonprofit hospital medians, fiscal 2024, released August 2025.
- Operating revenue growth: 9.3%
- Operating expense growth: 7.3%
- Operating cash flow margin: 6.3%
- Medicare as a percentage of gross revenue: 48.3%
- Medicare managed care as a percentage of gross revenue: 22.4%
- Inpatient admissions growth: 4.8%
- Outpatient surgery volume growth: 2.7%
- Emergency room visit growth: 4%
Revenue, expense and volume trends
Source: Kaufman Hall National Hospital Flash Report March 2026 data (published May 18, 2026), sampled from more than 1,300 hospitals. Figures are national medians; percentages are year-over-year (March 2026 vs. March 2025) unless noted.
- Calendar-year-to-date operating margin, including allocations: 1.7%
- Net operating revenue per calendar day: up 8%
- Gross operating revenue per calendar day: up 10%
- Inpatient revenue per calendar day: up 7%
- Outpatient revenue per calendar day: up 12%
- Net patient service revenue per adjusted discharge: up 4%
- Net patient service revenue per adjusted patient day: up 6%
- Bad debt and charity care per calendar day: up 18%
- Bad debt and charity care per calendar day, first-quarter year-to-date: up 15%
- Bad debt and charity care as a percentage of gross operating revenue: up 5%
- Total expense per calendar day: up 7%
- Labor expense per calendar day: up 4%
- Non-labor expense per calendar day: up 10%
- Supply expense per calendar day: up 11%
- Drug expense per calendar day: up 10%
- Purchased-service expense per calendar day: up 8%
- Full-time equivalents per adjusted occupied bed: down 8%
- Discharges per calendar day: up 1%
- Adjusted discharges per calendar day: up 4%
- Average length of stay: down 3%
- Emergency department visits per calendar day: up 1%
- Operating room minutes per calendar day: up 6%
- Outpatient revenue per calendar day, 500-plus bed hospitals: up 16.8%
- Illustrative 60/40 investment portfolio return: -4.9%
- Healthcare municipal bond issuance, year-to-date through early April 2026: $12.5 billion
Average adjusted expenses per inpatient day
Source: KFF / Kaiser State Health Facts, based on the 2024 American Hospital Association Annual Survey.
- Nonprofit hospitals: $3,449
- For-profit hospitals: $2,623
- State/local government hospitals: $3,089
The post 100 hospital financial benchmarks | 2026 appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
41 hospital jobs ranked by share of healthcare workforce
Nearly 1 in 5 healthcare workers in the U.S. is a registered nurse, according to May 2025 data from the Bureau of Labor Statistics. RNs account for about 19% of the nation’s combined healthcare practitioner and healthcare support workforce — a larger share than any other single occupation.
Below are 41 hospital occupations ranked by their share of the healthcare workforce, based on BLS Occupational Employment and Wage Statistics data released May 15.
Editor’s note: Percentages reflect each occupation’s share of total combined employment in healthcare practitioner and technical occupations and healthcare support occupations (17.7 million workers nationally), per May 2025 BLS Occupational Employment and Wage Statistics data. The figure in parentheses is each occupation’s total national employment across all industries. For occupations not classified by BLS as healthcare roles — including security guards, housekeeping cleaners, cooks and chaplains — hospital-specific employment was used in place of total national employment to calculate the percentage. All figures exclude self-employed workers. The list is not exhaustive.
| Occupation | Share of healthcare workforce | Total national employment |
| Registered nurses | 19.07% | 3,379,720 |
| Nursing assistants | 8.17% | 1,448,910 |
| Medical assistants | 4.61% | 817,870 |
| Licensed practical and licensed vocational nurses | 3.66% | 648,410 |
| Medical and health services managers | 3.37% | 597,080 |
| Pharmacy technicians | 2.66% | 471,680 |
| Clinical laboratory technologists and technicians | 1.88% | 332,940 |
| Nurse practitioners | 1.82% | 323,040 |
| Pharmacists | 1.82% | 321,970 |
| Physical therapists | 1.51% | 267,330 |
| Radiologic technologists | 1.30% | 230,490 |
| Medical records specialists | 1.10% | 194,720 |
| Healthcare social workers | 1.06% | 187,630 |
| Emergency medical technicians | 1.02% | 180,510 |
| Occupational therapists | 0.92% | 162,450 |
| Physician assistants | 0.91% | 162,150 |
| Phlebotomists | 0.81% | 143,540 |
| Respiratory therapists | 0.79% | 139,790 |
| Surgical technologists | 0.66% | 117,460 |
| Family medicine physicians | 0.61% | 107,510 |
| Paramedics | 0.57% | 100,610 |
| Diagnostic medical sonographers | 0.51% | 90,160 |
| Maids and housekeeping cleaners | 0.46% | 80,780 |
| Dietitians and nutritionists | 0.44% | 77,570 |
| General internal medicine physicians | 0.38% | 67,150 |
| Orderlies | 0.30% | 43,940 |
| Nurse anesthetists | 0.29% | 51,840 |
| Security guards | 0.28% | 49,340 |
| Pediatricians (general) | 0.22% | 39,390 |
| Anesthesiologists | 0.22% | 38,760 |
| Health information technologists and medical registrars | 0.22% | 38,100 |
| Emergency medicine physicians | 0.19% | 32,880 |
| Cooks | 0.17% | 30,550 |
| Psychiatrists | 0.16% | 27,980 |
| OB-GYNs | 0.12% | 21,260 |
| Cardiologists | 0.10% | 17,290 |
| Nuclear medicine technologists | 0.10% | 17,080 |
| Orthopedic surgeons (except pediatric) | 0.08% | 14,100 |
| Dermatologists | 0.06% | 11,370 |
| Physicians, pathologists | 0.06% | 11,110 |
| Chaplains (classified by BLS under clergy) | 0.05% | 9,220 |
The post 41 hospital jobs ranked by share of healthcare workforce appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
‘Provider’ vs. ‘physician’: What federal law actually says and why it’s so hard to change
The word “provider” has become a contested term in American medicine, and the pushback is intensifying.
In February, the American College of Physicians published a policy paper in Annals of Internal Medicine, arguing that referring to physicians as “providers” is not just imprecise but an ethical problem. The ACP’s Ethics, Professionalism and Human Rights Committee concluded that the term undermines physicians’ clinical accountability, blurs distinctions in training and expertise, and erodes the physician-patient relationship by making it transactional. “The words physician and provider are not interchangeable,” the paper stated.
The AMA has held a similar position for years. Existing AMA guidance prohibits the medical association from using the term to refer to physicians in its own publications and calls on healthcare entities to use clinicians’ recognized titles and credentials in contracts and communications. At its Annual Meeting June 5-10 in Chicago, the AMA’s House of Delegates took this a step further, voting to formally oppose use of the term “provider” when referring to physicians.
A closer look at the term’s origin in U.S. healthcare highlights why unwinding it may be more complicated than retiring a word. “Provider” entered federal health policy with the Social Security Amendments of 1965, which created Medicare and Medicaid. In the original statute, the term referred specifically to institutional entities (hospitals, extended care facilities and home health agencies) that received payment from the federal government. Physicians were addressed separately under their own defined category, “medical and other health services,” in Section 1861(s) of the Social Security Act.
Over subsequent decades, as Medicare and Medicaid expanded to cover additional practitioners, including physician assistants, nurse practitioners and clinical social workers, the term broadened in practice. In billing systems and common usage, “provider” came to describe any individual or entity eligible to receive reimbursement. The statute’s own definition of “provider of services” never changed to include individual physicians. In Medicare law, physicians fall under a separate category, “suppliers,” defined as distinct from providers of services.
Perhaps no single regulatory change illustrates the drift more concretely than CMS’ renaming the 10-digit number clinicians and healthcare organizations use to submit claims to Medicare from the “Unique Physician Identification Number” to the “National Provider Identifier” in 2007.
Retiring “provider” from federal health policy would mean touching CMS rulemaking across dozens of programs, HIPAA transaction standards that govern the NPI system, the contracts of every major commercial insurer that mirrors federal language and state Medicaid programs in all 50 states.
The debate signals a tension between the administrative architecture of the federal healthcare payment system and the clinical identity of the workforce it covers — one that is unlikely to resolve quickly.
The post ‘Provider’ vs. ‘physician’: What federal law actually says and why it’s so hard to change appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
States with the highest, lowest APP job growth
Among four advanced practice provider positions, only nurse practitioners saw growth in employed workers between 2024 and 2025.
The Bureau of Labor Statistics reports on the number of employed people in each roll by state. The data, released May 13, calculated the number of employed people in 2025. Becker’s gathered data for all of the APP positions that the bureau tracks.
Between 2024 and 2025, physician assistants saw a decline of 0.3%, or 550 positions, in the number of employed staff, while nurse anesthetists saw a 9% decline. Nurse practitioners, however, saw an increase of 0.8%, or 2,630 positions. Nurse midwives saw a 16.4% decline, but that could be due to a number of states not reporting totals of employed midwives.
Here are the states and the District of Columbia with the number of employed APPs in 2025.
Editor’s note: “NA” indicates that BLS did not report the number of employed positions. If there was no data for either 2024 and 2025, Becker’s put NA for the total change.
| State | Physician assistants | Nurse anesthetists | Nurse practitioners | Nurse midwives | ||||
| Total employed 2025 | % change from 2024 | Total employed 2025 | % change from 2024 | Total employed 2025 | % change from 2024 | Total employed 2025 | % change from 2024 | |
| Alabama | 930 | 20.8% | 1,810 | 28.4% | 5,640 | 19.2% | NA | NA |
| Alaska | 700 | 4.5% | 90 | 200% | 710 | 24.6% | 60 | 0% |
| Arizona | 3,750 | 5.9% | 310 | NA | 7,220 | -4.2% | 80 | 0% |
| Arkansas | 850 | -12.4% | NA | NA | 3,970 | 18.5% | NA | NA |
| California | 13,600 | 0.2% | 2,230 | -1.8% | 25,120 | 19.7% | 870 | -1.1% |
| Colorado | 3,270 | 2.8% | 800 | 27% | 4,270 | 3.4% | 180 | -14.3% |
| Connecticut | 3,570 | -3.5% | 480 | -15.8% | 3,750 | 1.9% | 150 | 50% |
| Delaware | 860 | 24.6% | NA | NA | 1,430 | 18.2% | NA | NA |
| District of Columbia | 470 | -24.2% | NA | NA | 680 | -13.9% | 70 | 0% |
| Florida | 9,310 | -11.9% | 4,600 | -25.1% | 21,790 | -11.7% | 460 | -46.5% |
| Georgia | 5,610 | 27.5% | 1,170 | 0.9% | 10,460 | -1.1% | 300 | -21.1% |
| Hawaii | 530 | 20.5% | NA | NA | 550 | 17% | NA | NA |
| Idaho | 1,320 | 12.8% | NA | NA | 1,750 | 11.5% | NA | NA |
| Illinois | 3,790 | -3.6% | 1,140 | -10.2% | 9,270 | -3% | 280 | -9.7% |
| Indiana | 2,110 | -1.9% | 600 | 71.4% | 7,450 | -0.3% | 170 | 70% |
| Iowa | 1,200 | 0% | 380 | -34.5% | 3,240 | 15.3% | 80 | 14.3% |
| Kansas | 890 | -11.9% | 910 | NA | 3,780 | 24.8% | NA | NA |
| Kentucky | 1,360 | 8.8% | 1,640 | 56.2% | 4,770 | 1.3% | NA | NA |
| Louisiana | 1,360 | -23.2% | 900 | 1.1% | 5,380 | 20.1% | 60 | NA |
| Maine | 1,030 | 10.8% | 380 | -15.6% | 1,650 | 1.2% | 50 | 0% |
| Maryland | 2,950 | 1% | 840 | 18.3% | 6,710 | 1.1% | 240 | -7.7% |
| Massachusetts | 4,470 | 3.7% | 500 | -18% | 8,070 | -9.5% | 280 | 47.4% |
| Michigan | 6,310 | 14.9% | 2,300 | -22.3% | 8,290 | 4.9% | 430 | 59.3% |
| Minnesota | 3,660 | -3.4% | 2,130 | -17.1% | 7,780 | -10.5% | 410 | 57.7% |
| Mississippi | 320 | -13.5% | 480 | 77.8% | 4,690 | 12.5% | NA | NA |
| Missouri | 2,300 | 39.4% | 1,550 | 28.1% | 7,710 | 13% | 80 | 33.3% |
| Montana | 600 | -1.6% | NA | NA | 1,260 | 20% | NA | NA |
| Nebraska | 1,330 | 6.4% | 430 | 48.3% | 2,340 | 8.8% | NA | NA |
| Nevada | 1,090 | -8.4% | NA | NA | 1,930 | -34.4% | NA | NA |
| New Hampshire | 1,060 | 0% | 490 | 145% | 1,770 | -1.1% | 60 | 20% |
| New Jersey | 4,790 | 102.1% | NA | NA | 9,950 | 3.8% | 120 | -36.8% |
| New Mexico | 700 | 9.4% | NA | NA | 1,770 | -5.3% | 50 | -61.5% |
| New York | 19,140 | -1.3% | 2,450 | 102.5% | 22,890 | 12% | 360 | -26.5% |
| North Carolina | 7,490 | -12.1% | 3,340 | 18.4% | 9,800 | 22.2% | 240 | -31.4% |
| North Dakota | 510 | -1.9% | 250 | 0% | 1,290 | 2.4% | NA | NA |
| Ohio | 4,900 | 8.2% | 2,300 | -6.5% | 15,400 | 5.8% | 180 | 20% |
| Oklahoma | 1,770 | -0.6% | 990 | NA | 3,620 | 19.9% | NA | NA |
| Oregon | 2,250 | 16.6% | 370 | -24.5% | 2,820 | 16% | 240 | -11.1% |
| Pennsylvania | 9,020 | 16.2% | 2,500 | -6% | 10,670 | -1.7% | 320 | -39.6% |
| Rhode Island | 810 | 35% | 120 | NA | 1,180 | -1.7% | 80 | -11.1% |
| South Carolina | 2,250 | 9.8% | 1,010 | 6.3% | 5,670 | -3.1% | 100 | 233.3% |
| South Dakota | 680 | 4.6% | 400 | 8.1% | 1,020 | 7.4% | NA | NA |
| Tennessee | 2,240 | -5.9% | 1,690 | -28.4% | 12,150 | -15% | 330 | 26.9% |
| Texas | 10,110 | 0.8% | 4,060 | 10.9% | 25,970 | 19.7% | 290 | -21.6% |
| Utah | 1,610 | -3.6% | NA | NA | 2,740 | -4.2% | 140 | 40% |
| Vermont | 410 | 0% | 40 | -20% | 700 | 2.9% | 60 | 50% |
| Virginia | 4,340 | 22.9% | 700 | -28.6% | 7,110 | 9.9% | NA | NA |
| Washington | 3,540 | 6.9% | 760 | 4.1% | 6,700 | 39.9% | 170 | 13.3% |
| West Virginia | 1,080 | 12.5% | 740 | -6.3% | 2,550 | 11.8% | NA | NA |
| Wisconsin | 3,580 | 17.8% | 990 | -4.8% | 5,160 | 4.2% | 200 | 122.2% |
| Wyoming | 330 | -19.5% | 80 | 0% | 440 | 0% | NA | NA |
The post States with the highest, lowest APP job growth appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Medicare Advantage spending flagged as hospital fund depletion moves up: 4 notes
The Hospital Insurance Trust Fund is estimated to pay full Medicare Part A benefits only through the second quarter of 2033, one quarter earlier than last year’s projection of the third quarter, according to the 2026 Social Security and Medicare Trustees Report published June 9.
Part A covers inpatient, skilled nursing, home health and hospice care services.
Four things to know:
- At depletion, the program would cover 89% of scheduled Part A benefits, falling to 85% by 2050 before recovering to 93% by 2100. The fund had $255.7 billion in reserves at the end of 2025, and annual fund deficits are projected to return in 2027.
- The trustees tied the worsening outlook in part to upward revisions in Medicare Advantage per capita spending, higher utilization and lower projected tax revenue from Social Security benefits following enactment of H.R. 1. The fund’s 75-year actuarial deficit widened to 0.56% of taxable payroll, up from 0.42% last year.
- The fund’s projected depletion date first moved to 2033 last year, pulled forward from a prior 2036 estimate.
- The trustees project Part D costs to be significantly higher than last year in every year of the projection, citing a 2025 surge in “certain specialty” drug usage, higher cost trends and lower rebates. The Supplementary Medical Insurance fund covering Parts B and D remains adequately financed indefinitely because premiums and federal contributions reset annually.
The post Medicare Advantage spending flagged as hospital fund depletion moves up: 4 notes appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
The emerging healthcare model leaders are flocking to
As the link between oral health and overall wellness becomes more widely recognized among patients, healthcare leaders are looking for more ways to integrate care to enhance patient outcomes.
More than 90% of adults in the U.S. agree that oral health is an important aspect of overall health, according to a new report from the Delta Dental Plans Association. Adults part of Gen Z are driving the increase, with 94% of Gen Z respondents believing that oral health is very or extremely important to their overall health, up from 89% in 2025.
Henderson, Nev.-based PDS Health, an integrated healthcare organization with more than 1,200 locations in 24 states, has been spearheading efforts to bring medical and dental care closer together, including partnering with hospitals and health systems to expand its primary care model.
Brett Bingham, president of PDS Health Medical, recently spoke with Becker’s to discuss its growing primary care model and how care coordination is enhancing the patient experience.
Note: Responses were lightly edited for clarity and length.
Question: Can you tell me about how PDS Health’s primary care model is structured and how it integrates dental and medical care?
Brett Bingham: PDS Health has built a modern primary care model alongside one of the largest DSOs in the world. The differentiator is not simply co-location. It’s really the combination of the care model, the data model, the technology and the patient experience organized around the reality that oral health and overall health are inextricably linked — what we call the Mouth-Body Connection.
Primary care is often treated as order takers and referral makers. Our model helps restore primary care as the front door to prevention, early detection, longitudinal care and affordability.
Our structure really has three core elements. First, we use PDS Health’s existing scale, infrastructure and patient relationships to expand access to medical care. Second, we integrate medical and dental through shared workflows, shared data, coordinated protocols [and] clinical handoffs. Third, we’re really focused on creating value for patients, providers, payers, employers and health systems. Ultimately, it has to work for everybody.
Epic serves as our platform across both dental and medical care, allowing clinicians to access integrated health records and coordinate care in ways many organizations discuss conceptually but struggle to operationalize. We’ve turned that into a practical operating model.
Q: What does coordinated care look like day-to-day between clinicians in this model? What does it look like for patients?
BB: I think the most important thing is that coordination has to be practical. Far too often in healthcare, we strategize about grandiose ideas that never come to [fruition], but it only creates value when it becomes part of everyday workflows, documentation, handoffs and cross-team communication.
In our co-located practices, medical and dental teams participate in shared huddles each morning and coordinated care protocols. Dental teams may identify elevated blood pressure, diabetes risk, sleep-related concerns, inflammation or other clinical indicators that warrant medical follow-up. Likewise, medical teams may identify patients who need periodontal care, oral health support or dental follow-up as part of managing chronic conditions. The goal is not to blur professional roles. Oral health providers, physicians and advanced practice providers each practice at the top of their license within a system designed to connect their work.
For patients, the experience is more seamless. Rather than being told to follow up elsewhere, care teams can often coordinate services while the patient is already in the practice. In many cases the patient can just walk across the hall to see the other provider while they’re there. The goal is for patients to feel that the team is focused on the whole person, not just treating one aspect of their body or another aspect of their care, such as a tooth or just a blood pressure reading. The idea is for our providers on both sides of the house to treat the whole patient and focus on overall health and help them with their entire healthcare journey.
Q: How can this model enhance early detection of systemic disease?
BB: Dental visits are a powerful touchpoint. Many patients see their dental team more frequently than they see their primary care provider, creating opportunities to identify clinical indicators that may warrant further evaluation, such as evidence of oral inflammation or hypertension.
The key is what happens next. Our model connects those findings through shared clinical protocols, documentation and coordinated follow-up. Whether it be in a CBCT scan or medical grade imaging, or other observations that surface at the point of care in the dental or primary care environment, the information can be connected to the appropriate care pathway.
We’ve seen examples where integrated dental-medical workflows led to the identification of potentially serious health concerns and expedited medical intervention. That’s where integration creates true value for patients and significantly improves health outcomes.
Q: How do you encourage medical and dental teams to think beyond their traditional silos?
BB: It starts with respect for both professions. Integration can’t feel like one side is subordinate to the other, and it’s not. Dental teams have deep patient relationships and identify important clinical signals, and primary care teams bring diagnoses, treatment and longitudinal disease management across the patient journey. Both are essential.
From there, we make the clinical case clear. Everybody in healthcare has a story about why they entered healthcare and why they do what they do. As we focus on oral health and overall health and how they’re inextricably linked, we’re able to connect that purpose across our providers and our team members.
Healthcare hasn’t historically been organized that way, but when teams understand the connection between oral health and broader health outcomes, the model becomes intuitive.
The operating model is equally important. We support integration through shared protocols, coordinated handoffs and workflows that make collaboration achievable. Most clinicians want to do the right thing for patients. Our job is to make integration easy, so it becomes a natural part of care delivery rather than an additional burden.
Q: How are you measuring success within this integrated care model?
BB: We evaluate success across several dimensions.
First is access. Across the U.S., primary care is needed in just about every community. One of the first pieces we’re looking at is whether each location expands primary care access in the market it’s serving.
The second is the patient experience. We’ve received very positive feedback from patients, which tells us they are responding well to the model.
The third is clinical integration. We’re measuring how effective our workflows connect and whether those pieces create a seamless encounter for the patient, rather than simply being co-located.
The fourth is provider engagement. Provider engagement among those already part of our organization has been strong, and interest from clinicians who want to participate in the model continues to grow. Just this week, I received a message from a nurse practitioner who shared how much she valued the model, the team and the culture and everything, and wanted to know how she could take the next step toward ownership. I found that incredibly encouraging because it reflects the enthusiasm we’re seeing from clinicians who believe in a more integrated approach to care.
The final piece is value. We have to demonstrate value for all stakeholders because, as we look to restore primary care, the model has to be meaningful, scalable, financially sustainable and ultimately better for patients.
Q: Who is PDS Health currently partnering with in the medical space for this model?
BB: PDS Health has a lot of rich connections and partners across the healthcare ecosystem. Recently, we signed an affiliation agreement with a large multi-state integrated delivery system in the West, which will be announced publicly in the near future.
We’re also in active discussions with a number of other health systems that are looking for new approaches to expanding access and improving care coordination.
Health systems continue to face challenges related to primary care access, reimbursement cuts and population health strategy. We believe our model offers a practical way to strengthen coordinated care within local markets.
We believe the model is highly complementary to health systems, and we’re actively exploring opportunities with organizations that share our vision for integrated care.
Q: Are you targeting specific areas where there are shortages of primary care and/or dental providers?
BB: As we consider our model and the connection points between oral health and medical health, we want to make sure we’re leveraging PDS Health’s strength. We’re looking at markets where PDS Health is already present and building from that ecosystem, while also considering who can partner well in that space, what the employer or payer environment looks like, and most importantly, what patients need. We are looking at primary care access scores because, ultimately, that’s where we can do the most good.
Q: How do you plan to expand this model down the line?
BB: We’ll continue to be disciplined in our growth strategy. The focus is not growth for growth’s sake, but thoughtful expansion into markets where we can create meaningful value for patients and the communities we serve.
Health system partnerships will continue to be an important part of that strategy. We see a significant opportunity to collaborate with organizations that are already serving communities and looking for new ways to expand access to coordinated care.
As far as where it goes from here, I think there’s a lot of opportunity for growth and a lot of value that can be created through a more connected model of care. I don’t want to put artificial limits on what that could become because the culture at PDS Health is phenomenal, and there are a lot of things we’ll be able to accomplish as we continue partnering with like-minded organizations and individuals. Ultimately, I believe we’re going to be able to do a lot of good for the healthcare community.
The post The emerging healthcare model leaders are flocking to appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
The 4.2x link between staff engagement and patient experience
Hospitals in the top quartile for employee engagement are 4.2 times more likely to achieve top patient experience scores, according to a Press Ganey report that analyzed feedback from more than 2.6 million healthcare employees and physicians surveyed in 2025.
The report found that employee engagement rose from 3.97 to 4.01 over the past year — the largest gain in eight years — while physician engagement climbed from 3.96 to 4.01. But Press Ganey cautioned the recovery remains fragile, with 35% of employees and 37% of providers lacking confidence in senior leadership.
The cost of disengagement is significant: Disengaged caregivers are 2.6 times more likely to leave. At the average health system, defined as one with 3,000 employees, turnover costs more than $16 million annually. Turnover rates at low-engagement organizations run at 24%, compared with 15% at high-engagement systems.
The report also flagged early warning signals that many organizations may be missing. Among employees who plan to leave within three years, 34% exit within one year. Additionally, 26% of survey nonrespondents leave within a year, compared with 15% of respondents — suggesting nonresponse itself is a meaningful attrition indicator.
Turnover pressure is concentrated at both ends of the workforce: Generation Z employees show the highest turnover rate at 35%, while baby boomer turnover is rising from 19% to 21%. Advanced practice providers remain among the least engaged groups, with Press Ganey citing gaps in role clarity and involvement in decision-making.
The post The 4.2x link between staff engagement and patient experience appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
10% increase in nurse responsibility improves retentions by 54%: Study
Nurses are less likely to leave when they have greater responsibility for patient care, according to an article published in Harvard Business Review.
The study followed 430 full-time ICU nurses at a large U.S. hospital over 26 months. Researchers analyzed data from the EHR to see nurses’ care activities, and used staffing, scheduling and HR data to determine the nurse workload on a granular level. The level of responsibility was defined as the number of patients a nurse was the primary provider for during a shift.
Here are the key findings:
1. A 10% increase in responsibility reduces the odds of quitting by more than 54%.
2. Nurses trusted with real responsibility reported feeling more central to the work on the unit, being seen by the organization as capable and important, and a deeper sense of ownership.
3. Nurses who received help from teammates during a shift had 40% lower odds of overtime-induced quitting and 22% lower work-pressure-triggered odds of quitting.
4. Leaders can apply these findings by training nurses to manage complex patients, operate sophisticated equipment and giving nurses latitude to use their clinical judgement.
The post 10% increase in nurse responsibility improves retentions by 54%: Study appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
20 most trusted health system brands
Austin-based UT Health Austin was named the most trusted healthcare brand in Monigle’s “2026 most trusted healthcare brands” section of its Humanizing Brand Experience Vol. 9 report.
Brand consultancy Monigle surveyed more than 3,000 nationally balanced U.S. healthcare consumers for the report, which examined trust, engagement, compassion and healthcare consumer sentiment.
Here are the 20 most trusted health system brands, according to the report:
- UT Health Austin
- Mayo Clinic (Rochester, Minn.)
- Emory Healthcare (Atlanta)
- Johns Hopkins Medicine (Baltimore)
- BayCare (Clearwater, Fla.)
- Penn Medicine (Philadelphia)
- Mass General Brigham (Somerville, Mass.)
- Duke Health (Durham, N.C.)
- Mount Sinai Medical Center (Miami Beach, Fla.)
- UCI Health (Orange, Calif.)
- UT Health San Antonio
- Bon Secours-St. Francis (Greenville, S.C.)
- UVA Health (Charlottesville, Va.)
- Virtua Health (Marlton, N.J.)
- University of Maryland Medical System (Baltimore)
- Hoag (Newport Beach, Calif.)
- Vanderbilt Health (Nashville, Tenn.)
- University of Iowa Health Care (Iowa City, Iowa)
- Penn State Health (Hershey, Pa.)
- UAB Medicine (Birmingham, Ala.)
The post 20 most trusted health system brands appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
How hospitals are fending off a retirement wave
While hospitals and health systems work to recruit and retain the next generation of healthcare talent, another group is also top of mind: those nearing retirement age.
A recent study found that leaving the workforce before retirement age may accelerate cognitive decline, and working into older ages could help delay it. For employers, the case for retaining experienced employees is also pressing amid concerns of a wave of baby boomer retirements that could thin institutional knowledge across the workforce.
To keep their most experienced team members engaged, health systems are building structured pathways that let them stay in the workforce longer, including flexible scheduling, phased transitions and mentorship programs.
At Annapolis, Md.-based Luminis Health, employee well-being is a top priority — including support for those approaching retirement, Chief Human Resources Officer Amy Beales told Becker’s. One area of focus has been encouraging earlier and more intentional retirement planning conversations between leaders and staff members.
“By discussing timing, scheduling flexibility, and phased transitions well in advance, we can adjust responsibilities or hours in ways that better support the employee while also helping the organization plan ahead,” Ms. Beales said. “In many cases, this approach has helped retain experienced employees longer, strengthen knowledge transfer and mentorship, and reduce operational gaps during leadership or staff transitions.”
Other systems are formalizing those transitions into structured programs. Santa Barbara, Calif.-based Cottage Health has made succession planning a key focus, CHRO Cara Williams told Becker’s in 2025, implementing a program that allows retiring employees to phase their retirement over two years while building a robust succession plan across all levels.
Nurses are a key focus. Morgantown, W.Va.-based WVU Medicine offers a work-life balance program that allows qualifying nurses near retirement to work part-time while receiving full-time benefits, a structure designed to boost retention, Assistant Vice President of System Nursing Services Jessica Huffman, DNP, RN, told Becker’s in September.
Physicians are also a top priority. They are leaving clinical practice earlier than ever as a result of stress and administrative burden, according to a May study conducted by American Medical Association researchers. The shift comes as the U.S. faces a projected physician shortage of between 13,500 and 86,000 by 2036 — a gap that could be reduced by about 40,000 simply by increasing the average retirement age by two years, the researchers found.
Physician CEOs have been especially focused on retaining later-career physicians, with many systems offering part-time roles and flexible schedules to meet their evolving needs.
At Duluth, Minn.-based Essentia Health, section leaders meet twice a year with the colleagues to discuss development, regardless of career stage, CEO David Herman, MD, told Becker’s in 2025. When one physician considering retirement said they would prefer to focus on inpatient work, and another at a similar stage wanted only outpatient work, Essentia restructured their duties to meet their needs.
“Suddenly they both said, ‘I think I have another five years left in me,’” Dr. Herman said. “The things that create energy are different for everyone.”
Beyond scheduling, systems are also opening up new paths for experienced physicians who want to stay involved in different ways. Richmond, Va.-based VCU Health, for instance, creates opportunities for physicians pursuing MBAs or transitioning into leadership roles. CEO Marlon Levy, MD, told Becker’s in 2025 that many physicians late in their careers are not looking to leave entirely.
“They want to continue to participate — often not either administratively or clinically, but both,” Dr. Levy said. “It’s incumbent upon administrative teams to understand that doctors feel like they may have more to contribute in the administrative or leadership space than they had in the past.”
The post How hospitals are fending off a retirement wave appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Where RNs are most concentrated: Rankings by state
Larger states such as California and Texas employ the highest number of registered nurses nationwide. But when measured by concentration — the number of RNs employed per 1,000 jobs in a state’s economy — both states rank much lower, according to May 2025 data released May 15 from the Bureau of Labor Statistics.
West Virginia had the nation’s highest RN concentration at 33.4 nurses per 1,000 jobs, while Utah ranked last at 15.8.
Nationwide, general medical and surgical hospitals employed the largest share of registered nurses, accounting for about 56% of RN employment, or roughly 1.9 million jobs. Physicians’ offices and home healthcare services employed the next-largest shares of RNs.
Below are the employment-per-1,000-job figures for registered nurses in all 50 states and the District of Columbia, according to BLS data.
1. West Virginia — 33.391
2. South Dakota — 32.170
3. Delaware — 29.478
4. North Dakota — 26.403
5. Missouri — 25.992
6. Ohio — 25.897
7. Maine — 25.827
8. Alabama — 25.707
9. Louisiana — 25.311
10. Kentucky — 25.144
11. Mississippi — 24.988
12. Vermont — 24.392
13. Massachusetts — 24.247
14. Pennsylvania — 24.161
15. Nebraska — 24.136
16. Michigan — 23.831
17. Minnesota — 23.766
18. Connecticut — 23.648
19. Kansas — 23.514
20. Florida — 23.156
21. Wisconsin — 23.138
22. Alaska — 23.057
23. Illinois — 22.780
24. Arizona — 22.581
25. Arkansas — 22.554
26. New Hampshire — 22.517
27. North Carolina — 22.486
28. Oklahoma — 22.409
29. Iowa — 22.077
30. Tennessee — 22.021
31. New Jersey — 21.624
32. South Carolina — 21.583
33. Indiana — 21.550
34. Montana — 21.410
35. New York — 21.244
36. Georgia — 20.648
37. New Mexico — 20.648
38. Hawaii — 20.622
39. Oregon — 20.198
40. Rhode Island — 20.132
41. Idaho — 19.690
42. Washington — 19.506
43. Texas — 19.287
44. Maryland — 19.149
45. Wyoming — 19.000
46. Colorado — 18.959
47. Virginia — 18.856
48. California — 18.609
49. Nevada — 17.447
50. District of Columbia — 16.305
51. Utah — 15.797
The post Where RNs are most concentrated: Rankings by state appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
VA security failed all 30 covert weapons tests: GAO
Department of Veterans Affairs staff did not detect a prohibited weapon that undercover Government Accountability Office investigators brought into any of 30 tested VA medical facilities — including two with metal detectors — according to a GAO report publicly released May 13.
Nine things to know:
1. The GAO was asked to review security at VA medical facilities. The report examines the nature of reported criminal activity at VA facilities, the extent to which the VA has implemented federal security requirements and detected vulnerabilities, and VA processes for incorporating security and threat information into infrastructure planning. GAO reviewed VA policies, crime data and risk assessment data; conducted covert tests at a non-generalizable sample of 30 facilities; and interviewed VA personnel and veterans in Arkansas and California.
2. VA staff also did not confront an investigator drinking in plain view from a bottle labeled vodka in 25 of 26 covert tests, which is generally prohibited at VA facilities.
3. The roughly 74,700 crimes reported at VA medical facilities in fiscal 2024 and 2025 were overwhelmingly nonviolent, including disorderly conduct, theft and drug offenses, according to the GAO’s analysis. The average crime rate over the two-year period was about twice as high at urban facilities (214 crimes per facility) than rural facilities (123 crimes per facility) — consistent with a Department of Justice report on overall criminal trends.
4. The Interagency Security Committee, of which the VA is a member, developed a risk management standard that federal agencies are required to follow. The GAO found the VA has not fully implemented all ISC requirements, including documenting decisions on the security strategies it will adopt or measuring the performance of those strategies.
5. The VA has a performance goal to address security gaps through capital planning, and while it has met its overall security-gap planning goal, two of 18 regions did not in fiscal years 2023 through 2025, the report said. GAO attributed this to VA headquarters not communicating to the regions that they were missing the goal.
6. GAO made three recommendations to the VA secretary: Develop a plan with milestones for fully implementing the ISC’s risk management standard; assess the resources needed to fully implement it; and develop a mechanism for VA headquarters to communicate with regional officials on their progress in meeting the 95% security gap closure planning goal.
7. A VA spokesperson told Becker’s in a May 20 statement that the “second Trump administration inherited from the Biden Administration a fractured VA police force plagued with problems,” adding that the VA identified many of the issues highlighted in the GAO report independently in early 2025 and has been working to fix them.
8. The spokesperson said successful efforts include establishing the Office of Security and Preparedness — led by its own assistant secretary — and consolidating VA police operations under that office. All VA police now report to a law enforcement professional with a direct line to the VA secretary’s office, an improvement from when VA police reported to nearly 150 different medical center directors, the spokesperson said.
9. The spokesperson also said the Trump administration worked with the Office of Personnel Management to reclassify VA police officers to qualify for higher pay, which is expected to improve recruitment, retention and upward mobility.
The post VA security failed all 30 covert weapons tests: GAO appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Penn Medicine operating income grows to $238M after Doylestown Health acquisition: 6 things to know
Philadelphia-based Penn Medicine reported an operating income of $238.5 million (2.4% margin) for the nine months ended March 31, up 46.3% from $163 million (1.9% margin) in the same period last year, according to financial documents filed May 20.
The results follow the April 1, 2025, acquisition of Doylestown (Pa.) Health. Doylestown Hospital, a 245-bed teaching hospital, became Penn Medicine’s seventh hospital and is now known as Penn Medicine Doylestown Health.
Six things to know:
1. Operating revenue climbed 15.2% year over year. Penn Medicine reported total operating revenue of $10.1 billion for the nine-month period, up from $8.8 billion during the same period in 2025. Net patient service revenue increased 13.5% year over year to $8.5 billion.
2. Expenses rose 14.9% year over year. Total operating expenses before interest, taxes, depreciation and amortization increased 14.9% year over year to $9.5 billion. Salaries and wages rose to $4 billion, while supplies and service costs increased to $4.1 billion. Interest expenses ($68.5 million) and depreciation and amortization ($335.3 million) costs dragged down the health system’s overall performance for the nine-month period.
3. EBITDA topped $642 million. Penn Medicine posted earnings before interest, taxes, depreciation and amortization of $642 million for the nine-month period, up from $540 million during the same period in 2025.
4. Net income rose sharply. Penn Medicine reported $748.2 million in net income, up from $431.2 million a year earlier. The increase was aided by $242.1 million in unrealized gains on alternative and equity investments and $183.1 million in net realized gains, contributions and other support.
5. The health system’s balance sheet expanded significantly. Total assets reached $17.2 billion as of March 31, 2026, compared with $15.4 billion a year earlier. Net assets grew to $10.7 billion from $9.7 billion. Long-term debt also increased, rising to $2.6 billion from $2.3 billion, reflecting capital investment activity during the period.
6. Volumes grew across several categories. Volume metrics reflect the Doylestown addition and underlying demand growth. Adult and neonatal admissions rose to 120,297 from 105,711 in the prior-year period. Emergency room visits increased to 370,992 from 332,307, and outpatient visits grew to 4.364 million from 3.938 million. Staffed adult and neonatal beds increased to 3,369 from 3,102, reflecting the addition of Doylestown Hospital’s 245-bed capacity. Occupancy held at 78%, up slightly from 77.5%.
The post Penn Medicine operating income grows to $238M after Doylestown Health acquisition: 6 things to know appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
RFK Jr. ousts 2 preventive services task force leads
HHS Secretary Robert F. Kennedy Jr. has removed the two vice-chairs of the U.S. Preventive Services Task Force, an expert panel that provides clinical preventive health recommendations to Congress, an HHS official confirmed to Becker’s May 21.
John Wong, MD, and Esa Davis, MD, led the task force. The group assigns grades to preventive services, which private health insurance covers without cost-sharing under the ACA.
According to documents obtained by Becker’s, the leaders were subject to a review under revised governance procedures, and the terminations did not stem from performance issues. The change comes just ahead of a May 23 nomination deadline for new members, and both are still able to apply.
The task force has been effectively sidelined for the past year, with its most recent meeting in March 2025. Since then, meetings have been postponed, with one cancellation occurring during the government shutdown. Last month, Mr. Kennedy said the volunteer group had been “lackadaisical and negligent” for two decades, adding it will meet more often than the planned three times per year.
“We strongly urge HHS to restore the USPSTF’s long-standing, transparent process for selecting members, specifically clinicians with expertise in the fields of preventive medicine and primary care,” a May 20 American Medical Association statement said. “We also implore HHS to commit to once again holding regular task force meetings to ensure its important work can continue without further delay. Our patients’ lives depend on it.”
Last year, HHS tried to overhaul the CDC’s Advisory Committee for Immunization Practices. Subsequent changes to the U.S. childhood vaccine schedule were met with a legal challenge. In April, the Trump administration filed notice that it would appeal the federal court ruling.
The post RFK Jr. ousts 2 preventive services task force leads appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Mayo Clinic in Florida receives $75M gift
Jacksonville-based Mayo Clinic in Florida has received a $75 million gift to support its expansion initiative.
Four things to know:
1. The donation from Paula and Randy Ringhaver will support the Lee Ringhaver Tower, a newly expanded hospital tower named in honor of the couple’s son, Randal “Lee” Ringhaver Jr., who died from leukemia in 1980 at 8 1/2 months old, according to a May 21 health system news release.
2. A five-story expansion of the tower began serving patients in 2025, adding 121 new rooms and digital technologies designed to support personalized care. The tower also includes shell space for future growth and capacity for three additional stories.
3. Including the Lee Ringhaver Tower expansion, Mayo Clinic’s “Bold. Forward. Unbound.” initiative encompasses more than 725,000 square feet of new clinical, research and education space. The initiative also includes the Duan Family Building, which contains the country’s’ first carbon ion therapy system, a biomanufacturing expansion and a future research and education building.
4. Across Mayo Clinic, “Bold. Forward. Unbound.” will add more than 4 million square feet of new space across campuses in Arizona, Florida and Minnesota.
The post Mayo Clinic in Florida receives $75M gift appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Former Kentucky system CEO dies
John Dubis, who spent more than 36 years in healthcare leadership, including as president and CEO of Edgewood, Ky.-based St. Elizabeth Healthcare, died May 14. He was 71.
During his tenure at the six-hospital system, Mr. Dubis was known for his integrity, compassion and vision, guiding the organization through continued growth and a commitment to high-quality patient care, according to his obituary.
Mr. Dubis joined St. Elizabeth Healthcare in 2007 as COO and was CEO from 2011 until his retirement in 2015 after a diagnosis of Parkinson’s disease.
St. Elizabeth Medical Center and St. Luke Hospitals merged to form St. Elizabeth Healthcare in late 2008, according to the system’s website. Mr. Dubis played a key role in the merger and, under his leadership, the system added 1,000 employees, improved operations and invested millions in facility improvements and new programs, The Enquirer reported Feb. 13, 2015.
Mr. Dubis discussed the merger in a 2012 interview with Smart Business, highlighting the need for clear communication, a patient-centered approach and adaptability amid a changing healthcare environment.
“It’s easy to get negative and pessimistic about what’s going to happen in the future. I frankly look at it as an opportunity to lead ourselves in a different way that could be even better than what we have today,” Mr. Dubis said. “This is a new world in which having a strong desire to embrace change and work within the abstract and uncomfortable zone of unfamiliarity is what it’s going to take to guide your organization to be successful down the road.”
Mr. Dubis also held executive leadership roles at several other hospitals and health systems, including SSM St. Mary’s Health Center in Jefferson City, Mo., SSM St. Francis Hospital and Health Center in Chicago, and SSM Cardinal Glennon Children’s Medical Center in St. Louis, according to his obituary.
He served on several boards and organizations, including the Kentucky Hospital Association and the Greater Cincinnati Health Council.
One comment on his obituary described him as a great mentor and friend during their years at St. Elizabeth. He will be remembered for his “steady presence, kind heart and deep dedication to helping others,” according to his obituary.
The post Former Kentucky system CEO dies appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Civica launches drug shortage program for 225 rural hospitals
The Civica Foundation has received a $3.2 million grant to launch a program aimed at expanding access to generic medications for rural hospitals in nine states.
The Civica Rural Hospital Program will support rural and critical access hospitals in Hawaii, Iowa, Minnesota, Montana, Nebraska, Nevada, North Dakota, South Dakota and Wyoming, according to a May 7 news release from the foundation. The initiative is designed to help hospitals secure access to generic medicines frequently affected by national drug shortages.
The three-year pilot program is expected to support approximately 225 rural hospitals representing an estimated 6,750 hospital beds. The Civica Foundation said grant funding will cover per-bed membership fees for eligible hospitals, allowing them to join Civica at no cost. Civica also said it will waive annual purchase commitments for participating hospitals.
The post Civica launches drug shortage program for 225 rural hospitals appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
Intermountain digital engagement VP steps down
Mona Baset, vice president of digital engagement at Salt Lake City-based Intermountain Health, is stepping down from her role.
Ms. Baset announced her departure in a May 20 LinkedIn post.
She has served in the role since April 2022. Ms. Baset said she will take a career break.
The post Intermountain digital engagement VP steps down appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
MetroHealth to roll out 500 smart rooms
Cleveland-based MetroHealth System plans to deploy smart technology at 500 patient rooms across five hospitals.
The public, safety-net health system intends to bring Artisight’s virtual nursing, virtual sitting and AI-powered fall monitoring and voice-command capabilities to its new Glick Center in Cleveland, hospitals in Brecksville, Cleveland Heights and Parma, and rehabilitation institute in Old Brooklyn over the next two years.
“Hospital smart rooms represent a shift toward patient-centered, technology-driven healthcare,” said Jill Evans, MSN, RN, chief nursing informatics officer and executive director of virtual care at MetroHealth, in a May 21 news release. “By automating tasks, improving safety, and enhancing comfort, these rooms enable providers to deliver more attentive and personalized care.”
MetroHealth selected the platform based on factors including staffing efficiency and cost reduction, faster discharges, fall rate reductions, HCAHPS score improvements, and caregiver satisfaction.
The post MetroHealth to roll out 500 smart rooms appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
States with the most, fewest licensed nurses per capita
The National Council of State Boards of Nursing found the District of Columbia has the most licensed nurses per capita, while Utah is the state with the fewest for the second year in a row.
The organization created a course of nursing licensure statistics in the U.S. and its territories. The data was compiled using the NCSBN’s database and Nursys, an electronic information system where regulatory bodies enter licensure data. All of the council’s 58 members shared licensure data, which amounted to 6,903,665 registered and practical nurses — up from 6,870,362 last year.
According to the data, Wyoming and Vermont had the fewest licensed nurses in their states overall, at 9,620 and 13,528, respectively. Meanwhile, California and New York had the most licensed nurses at 708,141 and 610,207, respectively.
Becker’s used 2025 Census data to calculate how many nurses are in each state per 100,000 population. Here are the five with the most and the five with the fewest nurses.
Most
| State | Total Nurses | 2025 population | Nurses per 100,000 |
| District of Columbia | 51,923 | 693,645 | 7,485 |
| Alaska | 23,138 | 737,270 | 3,139 |
| New York | 610,207 | 20,002,427 | 3,051 |
| Minnesota | 156,970 | 5,830,405 | 2,693 |
| Massachusetts | 191,320 | 7,154,084 | 2,674 |
Fewest
| State | Total Nurses | 2025 population | Nurses per 100,000 |
| Utah | 49,500 | 3,538,904 | 1,399 |
| Washington | 116,988 | 8,001,020 | 1,462 |
| Georgia | 177,673 | 11,302,748 | 1,572 |
| Idaho | 31,942 | 2,029,733 | 1,574 |
| Texas | 529,511 | 31,709,821 | 1,670 |
The post States with the most, fewest licensed nurses per capita appeared first on Becker’s Hospital Review | Healthcare News & Analysis.
‘Real consequences for access to care’: CMS’ $775B plan to cut Medicaid funding alarms hospitals
CMS’ latest proposal to cap certain state Medicaid payments has drawn immediate pushback from hospital groups, which argue the plan will further decrease access to care and destabilize hospitals that rely on supplemental Medicaid funding.
The agency proposed a rule May 20 that would create new limits for Medicaid state-directed payments and certain fee-for-service payments, aligning them more closely with Medicare rates. CMS said the proposed changes would reduce Medicaid spending by more than $775 billion over 10 years, including $510 billion in federal savings.
Under the proposal, CMS would cap certain state-directed payments for hospital, nursing facility and qualified practitioner services at academic medical centers at 100% of Medicare rates in Medicaid expansion states and 110% of Medicare rates in nonexpansion states for rating periods beginning on or after July 4, 2025. The agency also proposed extending the payment rate limit to all state-directed payments for all services in all states, the District of Columbia and territories for rating periods beginning on or after Jan. 1, 2029.
The American Hospital Association questioned how the policy would be implemented and how it could affect providers’ ability to rely on Medicaid payments.
“Healthcare-related taxes and Medicaid supplemental payment programs are longstanding tools that help address chronically inadequate base Medicaid payment rates, and the changes to these financing systems and related provider payments will have very real consequences for access to care in communities across the nation,” Ashley Thompson, senior vice president for public policy analysis and development at the AHA, said in a May 20 statement. “Projected reductions in funding for essential healthcare services will not only limit access to care for Medicaid patients. When hospitals and providers are forced to reduce services — or even close entirely — everyone in a community is impacted.”
America’s Essential Hospitals also criticized the proposal, arguing it would cut state-directed payments by hundreds of billions of dollars more than the Congressional Budget Office projected.
“CMS’ proposed cuts to state-directed payments go far beyond what Congress intended,” Jennifer DeCubellis, president and CEO of America’s Essential Hospitals, said. “By cutting SDPs by hundreds of billions of dollars more than the Congressional Budget Office projected, CMS will devastate essential hospitals’ ability to provide high quality care to the patients and communities they serve.”
Ms. DeCubellis added that Medicaid state-directed payments are a “financial lifeline” for essential hospitals and help states improve access to care for vulnerable patients.
The Federation of American Hospitals also urged CMS to work with hospitals as it advances the proposal.
“Patients rely on their local hospital to be there for them whenever they need care,” Charlene MacDonald, president and CEO of the Federation of American Hospitals, said in a statement. “A strong, sustainable Medicaid program is essential to maintaining that commitment, especially in rural areas where hospitals are often the largest employer and the only source of care for miles, and state directed payments are a critical part of that equation.”
The proposed rule includes a 60-day comment period. The AHA said it plans to issue a regulatory advisory to members detailing the proposal.
The post ‘Real consequences for access to care’: CMS’ $775B plan to cut Medicaid funding alarms hospitals appeared first on Becker’s Hospital Review | Healthcare News & Analysis.

What to Expect When Working for a Nurse Staffing Agency
Starting a new nursing job in metro Atlanta—or anywhere in Georgia, South Carolina, Alabama, Florida or beyond —can feel overwhelming, even when you know it’s the right move. Working for a nurse staffing agency opens the door to exciting opportunities like travel nursing jobs, per diem nursing positions, and flexible contract nursing assignments, but for many nurses, the process can seem mysterious.
Here’s what to expect and how to prepare so you can start your journey with confidence.
Whether you’re interested in contract nursing jobs, per diem, or full-time placements, the process of joining a nursing agency is straightforward.
- Explore Open Positions
Start by browsing our current healthcare staffing opportunities, including travel nurse contracts and per diem RN jobs across Georgia. You can view all available positions [here]. - Apply and Submit Your Resume
Once you find a role that matches your skills and interests—like emergency department nursing jobs, radiology technologist positions, or ICU contract assignments—submit your application. Our recruitment team reviews your resume to ensure a great fit. - Complete Skills Assessments
After initial screening, you’ll complete online assessments to evaluate your clinical expertise. - Interview and Client Screening
Next, you’ll interview with a recruiter from Staff Relief. Some positions require additional interviews with the hiring facility, especially for rapid response nursing or specialized roles.
The good news? This process typically moves fast—most candidates receive an offer within 9 days of applying.
More Earning Potential
One of the biggest reasons nurses choose agencies like Staff Relief is the pay. Per diem and contract nursing jobs can pay up to 50% more than traditional staff positions. You’ll also have access to the same premium assignments available with leading partners such as Aya Healthcare, AMN Healthcare, and Medical Solutions.
More Flexibility and Freedom
When you work with a nurse staffing agency, you decide when and where you want to work. Whether you prefer travel nurse assignments across the Southeast or local shifts around Georgia, you have control over your schedule.
More Responsibility and Professional Growth
As a contract or per diem nurse, you’ll take on additional responsibilities like tracking time and attendance. While this requires organization, it also builds valuable skills in accountability and independence.
More Variety and Travel
You won’t be tied to one facility. With travel nursing jobs, you can explore new cities, gain diverse experience, and enjoy housing assistance coordinated through agency partnerships.
More Security and Benefits
Even though you’re working flexible assignments, you still receive comprehensive benefits. Staff Relief provides health insurance and other perks so you can feel secure in your role.
If you’re a nurse who thrives in a fast-paced, dynamic environment and values more freedom, higher pay, and a variety of assignments, agency work could be your ideal career path.
Staff Relief partners with major healthcare staffing leaders to offer you access to top contracts and exclusive opportunities. Ready to get started?Contact Staff Relief today to learn more about our per diem nursing jobs, travel nurse assignments, and allied health contracts in Georgia. Let the best nurse staffing agency in Geogia find the perfect fit for your skills and goals.

Travel Nurse Pay in Georgia – Updated
Working as a contract nurse or per diem nurse in Georgia opens doors to flexibility, premium pay rates, and the chance to grow your experience across different healthcare settings. Whether you’re comparing travel nursing jobs, exploring remote RN jobs, or looking into per diem nursing positions, it’s essential to understand the factors that impact your earnings so you can make informed decisions and advocate for fair compensation.
Below, you’ll find everything you need to know about travel nurse pay in Georgia, average hourly rates, and how variables like specialty and location shape your paycheck.
When you partner with a nursing staffing agency or medical staffing agency, you’ll likely choose between contract assignments and per diem shifts:
- Contract Nursing Jobs: You’ll sign an agreement to work a set number of hours over a defined period, such as 8–13 weeks. Many contract nursing jobs offer guaranteed hours, premium rates for urgent needs, and stipends for housing and travel.
- Per Diem Nursing Jobs: “Per diem” means “per day.” These shifts are typically scheduled a week at a time, providing maximum flexibility for nurses who prefer short-term or occasional work. Per diem nurses often receive higher hourly rates to compensate for the lack of long-term commitment and benefits.
Whether you’re drawn to the stability of a contract or the freedom of per diem nursing shifts, you’ll be paid hourly, with rates that can fluctuate based on demand and specialty.
No two assignments are exactly the same. Here are the main factors that determine what you’ll earn as a travel nurse or per diem nurse in Georgia:
1. Location
Urban areas like Metro Atlanta and Savannah typically offer higher compensation compared to rural hospitals and clinics. Travel nurse jobs in Atlanta often pay a premium to attract experienced RNs to high-volume facilities.
2. Specialty
Your area of expertise makes a significant difference. Roles in the emergency department, ICU, operating room, and critical care nursing often command the highest hourly rates. Specialized skills like medical imaging, radiology technologist jobs, or dialysis RN contracts can further boost your earning potential.
3. Experience and Credentials
More years in the field—and specialty certifications—qualify you for higher-paying assignments. Rapid response nursing jobs and crisis response contracts also tend to pay more due to urgency and complexity.
4. Facility Type
Pay can vary depending on whether you’re working in an acute care hospital, skilled nursing facility, outpatient clinic, or rehab center. Some settings offer incentives like retention bonuses or completion bonuses.
5. Travel Requirements
Assignments requiring you to commute 50+ miles often include additional stipends or elevated pay rates to offset costs and time away from home.
While rates fluctuate weekly based on demand and season, here’s what you can generally expect in Georgia:
- General RN: $40–$46 per hour
- General RN (Metro Atlanta): $48–$55 per hour
- Specialty RN (ICU, OR, ED): $55–$75+ per hour, depending on urgency and shortage areas
- Licensed Practical Nurse (LPN): $25–$40 per hour
- LPN (Metro Atlanta): $30–$45 per hour
These figures often include travel stipends and housing allowances. For high-paying travel nursing companies or crisis response contracts, rates can exceed $80 per hour in peak demand.
Some agencies bundle housing and travel reimbursements, while others pay a higher hourly rate without stipends.
Before accepting a contract, review details carefully:
- Hourly base pay
- Housing allowance or provided housing
- Meal and incidentals stipends
- Travel reimbursements
- Completion and referral bonuses
If you’re unsure whether a pay package is competitive, compare it with similar contract nursing jobs.
- Get certified in high-demand specialties like emergency room nurse staffing, ICU nursing, or radiology technologist work.
- Consider rapid response nursing or ICU contract nurse positions for premium rates.
- Pick up flexible options like weekend nursing contracts or extra per diem shifts to maximize income.
- Keep your licenses and certifications current to qualify for the broadest range of assignments.
If you’re ready to explore per diem nursing jobs in Georgia or secure a travel nurse contract with competitive pay and benefits, Staff Relief, Inc. is here to help.
Contact us today to learn more about available contracts and start earning what you deserve.

The Ultimate Guide to Per Diem and Travel Nursing Jobs in the Southeast
If you’re an RN exploring your next career move, you’re not alone. Demand for per diem nursing jobs, travel nursing assignments, and contract nursing positions continues to rise across the Southeast—including Georgia, Florida, Alabama, and North Carolina.
At Staff Relief, we specialize in connecting nurses with flexible, rewarding opportunities at top healthcare facilities. Whether you’re searching for remote RN jobs, weekend nursing contracts, or emergency department nursing careers, this guide will help you understand your options and how to get started.
Per diem nursing offers unmatched flexibility. You can pick up shifts on your schedule—ideal for maintaining work-life balance or supplementing your income. Contract nursing jobs, meanwhile, provide stability for a set duration, often with higher pay rates and benefits.
- Flexible nursing shifts that fit your lifestyle
- The ability to work in acute care, skilled nursing facilities, or inpatient care units
- Opportunities to gain experience in critical care, emergency departments, or medical imaging
- Access to rapid response nursing jobs and crisis response travel nurse contracts that offer premium compensation
- The chance to build your resume with respected employers like Aya Healthcare, AMN Healthcare, and Medical Solutions
Many nurses are drawn to the Southeast for its competitive pay and growing healthcare networks. Here are some popular areas to consider:
- Georgia: From Atlanta to Savannah, per diem nursing jobs in Georgia are in high demand. If you’re wondering how to become a travel nurse in Georgia, Staff Relief can guide you through licensing and onboarding.
- Florida: Coastal communities and urban hospitals alike need RNs for contract nursing jobs in Florida, especially in ICU, OR, and emergency room nurse staffing.
- North Carolina: Explore travel nurse assignments in North Carolina, including rapid response nursing and critical care contracts.
- Alabama: More facilities are offering remote RN jobs in Alabama and local contracts to address staffing shortages.
You have more options than ever to search for your next role. While many nurses and allied health professionals look on popular platforms like Indeed and Vivian, applying through multiple agencies can be time-consuming and repetitive.
Staff Relief makes it simpler. Our job board and mobile app put thousands of opportunities in one place. You can browse, compare, and apply to positions without juggling multiple applications or credentialing processes.
Here are a few resources to explore:
- Staff Relief Job Board & Mobile App – Your all-in-one hub for per diem, travel, and contract jobs, with a streamlined application process and dedicated support.
- Indeed – Search a wide range of listings for nursing and allied health jobs.
- Vivian Healthcare Jobs – Compare pay packages and contract details across agencies.
Ready to save time and find your next assignment faster? Start with Staff Relief’s platform for the most efficient experience
Aya Healthcare, AMN Healthcare, and Medical Solutions are some of the most respected companies in the industry offering extensive travel nursing, per diem, and rapid response assignments nationwide. As a partner, Staff Relief has access to some of the same contracts and exclusive opportunities available through Aya, AMN, and Medical Solutions. You can explore top-paying positions without having to apply separately to multiple agencies. Whether you’re interested in Aya Healthcare contracts, AMN Healthcare rapid response nursing jobs, or Medical Solutions travel nurse assignments, our team can help you compare options and secure the role that fits you best.
Choosing the right nursing agency is essential. Whether you’re evaluating Aya Healthcare reviews, AMN Healthcare pay packages, or Medical Solutions job openings, here are factors to consider:
- Transparent pay packages and benefits
- Support with licensing and credentialing
- Access to crisis response contracts and rapid response nursing jobs
- A reputation for placing nurses in top paying travel nursing companies
- Ongoing support and career development resources
Staff Relief partners with major systems and local facilities to deliver healthcare staffing solutions that prioritize both the nurse and the patient.
If you’re searching for flexible RN shifts, contract nursing jobs, or remote nursing positions, we’re here to help. From emergency department nurse jobs to radiology technologist staffing, our team can match you with assignments that fit your goals.
Connect with Staff Relief today to get personalized recommendations, compare contracts, and start your next chapter with confidence.

Pros and Cons for Working for a Nurse Staffing Agency
In today’s fast-changing healthcare landscape, more nurses are exploring flexible career paths, including per diem nursing jobs, travel nursing contracts, and remote RN positions. Whether you’re a seasoned nurse searching for higher pay or a new grad eager to explore diverse settings, working with a nursing staffing agency can be a rewarding option. But like any career move, it’s important to weigh the benefits and challenges before deciding.
Below, we break down the main pros and cons of working with a medical staffing agency in Georgia and across the Southeast, so you can make the best choice for your lifestyle and goals.
One of the top reasons nurses choose per diem nursing positions or local contract nursing is the freedom to control their schedule. Unlike full-time hospital roles, contract assignments and per diem shifts let you decide when and where you work. This flexibility is ideal if you have family commitments, are pursuing further education, or simply want more autonomy in your day-to-day life.
Agencies like Aya Healthcare, AMN Healthcare, and Medical Solutions often post weekend nursing contracts, PRN RN positions, and rapid response nursing jobs you can pick up on your terms.
If maximizing your earnings is a priority, you’ll be glad to know that contract nursing jobs and per diem shifts typically pay higher hourly rates compared to permanent staff roles. These assignments often include stipends for meals, lodging, and travel—especially for travel nurse jobs in Atlanta, Savannah, and the Florida Panhandle. Many nurses find that with smart budgeting; they can work fewer shifts while maintaining or even increasing their income.
Plus, expenses related to travel nursing—like transportation and temporary housing—are often tax-deductible, creating additional financial benefits.
For nurses who thrive on change, working with a healthcare staffing agency provides a steady stream of new experiences. You’ll build your skills across different units, such as emergency departments, inpatient care, and even specialized areas like radiology technologist jobs or diagnostic imaging. This variety not only helps you stay engaged but also makes your resume stand out to future employers.
While flexible shifts are a major perk, it’s important to recognize that per diem nursing jobs don’t always guarantee steady hours. You may have weeks packed with back-to-back assignments, followed by slower periods. In some cases, last-minute schedule changes can impact your plans. If you prefer consistency, consider long-term contract nursing jobs, which often range from 6 to 17 weeks and offer more predictable schedules.
Contract and travel nurses frequently rotate among facilities, from skilled nursing facilities to acute care hospitals. Each location has its own protocols, electronic health records, and workplace culture. While you’ll eventually become comfortable in new settings, the learning curve can feel steep, especially when starting out. Nurses who value long-term relationships with coworkers and patients may find this aspect challenging.
If you’re adaptable, resourceful, and excited by the idea of working in diverse environments, you’re well-positioned to succeed. Many RNs say contract work rekindled their passion for patient care, exposed them to innovative treatments, and expanded their professional networks.
Whether you’re interested in remote nursing jobs in Alabama, ICU travel nurse assignments in Georgia, or emergency room contracts throughout the Southeast, there’s no shortage of options through reputable agencies like Aya Healthcare, AMN Healthcare, and Medical Solutions.
Ready to explore per diem nursing positions or contract opportunities? Here are a few steps to begin:
- Research Top Agencies: Read reviews and compare pay packages, benefits, and housing support.
- Set Your Priorities: Decide what matters most—schedule flexibility, pay rate, location, or specialty.
- Prepare Documentation: Update your licenses, certifications, and resume.
- Search Nursing Jobs Online: Use platforms like Indeed, Vivian Health, and agency job boards to find assignments that match your goals.
- Ask Questions: Speak with recruiters to understand expectations, cancellation policies, and support resources.
Working with a nursing staffing agency can be an empowering way to build a flexible, well-paid, and fulfilling career. If you’re considering making a change, take time to explore your options and connect with agencies committed to supporting nurses at every step.
Explore current per diem and contract openings with Staff Relief today and discover how flexible nursing can work for you.
How to Get a High Paying Contract Nursing Job
Contract nursing offers the chance to do meaningful work, gain diverse experience, and earn competitive pay. Whether you’re pursuing contract nursing jobs, per diem nursing positions, or rapid response assignments, the key to maximizing your income is preparation and strategy.
If you’re ready to secure a high-paying contract nursing job, use these proven tips to set yourself apart and negotiate pay that reflects your expertise.
Your resume is your first impression. A clear, polished resume highlights your skills, certifications, and professional accomplishments, and it determines whether you’ll be invited to interview.
Include:
- Your nursing specialties (such as ICU, emergency department, or medical imaging)
- Certifications (like ACLS, BLS, or specialty credentials)
- Details about your experience in different care settings, such as inpatient care, skilled nursing facilities, or acute care staffing
It’s normal to have employment gaps but be ready to confidently explain them during interviews. A well-organized resume positions you as a serious professional ready for high-paying nursing contracts.
Keeping your credentials updated makes you a more attractive candidate and can improve your earning potential.
Make sure to:
- Renew essential licenses and certifications promptly.
- Consider adding specialty certifications that are in demand for travel nursing jobs and contract assignments.
- Stay up to date with immunizations required by hospitals and clinics. Being ready with all documentation can speed up onboarding and help you access crisis response nursing jobs or urgent needs contracts that often pay premium rates.
The more prepared you are, the easier it is for a nurse staffing agency or recruiter to match you with higher-paying positions.
Professional references can be the deciding factor in landing a top-paying assignment.
Employers and recruiters rely on references to verify your:
- Clinical skills
- Professionalism
- Reliability
Choose references who can confidently speak to your work ethic and performance. Positive recommendations can open the door to flexible nursing shifts, per diem contracts, and specialized roles that pay more.
Flexibility is often rewarded in the world of contract nursing.
Consider these options to boost your pay:
- Accepting night shifts or weekends, which usually come with higher hourly rates.
- Taking assignments in locations experiencing shortages, such as rural facilities or emergency department nursing jobs.
- Being open to rapid response contracts or crisis response assignments, which often offer premium compensation.
When you demonstrate a willingness to adapt, you make yourself more valuable to medical staffing agencies and healthcare employers.
In contract nursing, your reputation follows you from one facility to the next. A strong track record makes it easier to secure higher-paying contracts and preferred assignments.
Tips for maintaining a great reputation:
- Be punctual and dependable.
- Communicate clearly with staffing agencies and supervisors.
- Go the extra mile to provide excellent patient care.
Facilities are willing to pay more to bring on nurses with proven reputations for excellence.
Being a contract nurse offers countless benefits, from career variety to premium pay. To make the most of your opportunities:
- Invest time in preparing a strong resume.
- Keep certifications and immunizations current.
- Maintain excellent references.
- Stay flexible with shifts and assignments.
- Build and protect your professional reputation.
When you combine preparation with dedication, you can consistently secure high-paying contract nursing jobs that match your skills and goals.
If you’re looking for your next opportunity, Staff Relief, Inc. is here to help. We partner with hospitals, clinics, and healthcare facilities to connect nurses with the best assignments in Georgia and beyond.
Contact us today to explore available contracts and start earning what you deserve.

How to Find the Best Nursing and Allied Health Jobs in 2025
If you’re thinking about a career change this year, you’re not alone. Thousands of nurses and allied health professionals are exploring contract nursing, per diem shifts, and even remote RN jobs to gain more flexibility, better pay, and fresh experiences.
But with so many options and so many staffing agencies—how do you know where to start?
This guide will walk you through:
✅ Why more professionals are choosing contract and per diem work
✅ How to evaluate agencies and read nursing agency reviews
✅ Where to find the best nursing jobs in 2025
✅ Tips for comparing assignments and getting hired faster
The days of sticking to one hospital job for your entire career are long gone. Today’s nurses are building more dynamic, customized careers—often combining contract assignments with per diem shifts.
The benefits of contract nursing are clear:
- Higher pay compared to permanent staff roles
- Housing and travel stipends
- Bonuses for completing assignments
- The chance to build experience in specialized areas like ICU, ER, and diagnostic imaging
- Flexibility to take time off between contracts
Meanwhile, per diem nursing jobs offer even more control over your schedule. You can pick up shifts when you want—whether that means extra weekends or just a few days a month.
If you’re drawn to this flexibility, you’re in good company. Contract and per diem work have become the fastest-growing segments of healthcare employment.
Once you decide to make a change, your next step is choosing a partner to help you find assignments. But not all agencies are the same.
Before you commit, take time to read nursing agency reviews. Here’s what to look for:
- Transparency in pay packages and benefits
- Support with licensing, credentialing, and onboarding
- Access to rapid response nursing jobs and high-demand contracts
- A track record of placing candidates in the highest paying travel nursing companies
- Clear communication and responsive recruiters
At Staff Relief, we know that trust matters. As a partner of Aya Healthcare, AMN Healthcare, and Medical Solutions, we can give you access to exclusive contracts without the hassle of applying to multiple platforms.
There are dozens of websites that list healthcare jobs, but it’s easy to get overwhelmed. To save time, start with the best nursing job sites for 2025:
- Staff Relief Job Board & Mobile App – Your one-stop platform to see per diem, contract, and travel nursing jobs nationwide, including remote RN jobs and medical imaging positions.
While many agencies focus on nursing alone, allied health roles are booming, too. If you’re a technologist or imaging specialist, consider exploring:
- Radiology technologist jobs in hospitals and outpatient centers
- Diagnostic imaging careers in high-demand specialties
- Medical imaging staffing agencies that can connect you to flexible contracts
- Radiographer employment for mobile imaging services or large health systems
Staff Relief supports professionals across disciplines and can help you find medical imaging jobs near you with excellent pay and benefits.
Ready to pick up extra shifts or transition into per diem work full-time? Here are tips to get per diem nursing jobs faster:
- Keep your credentials and health records updated.
- Sign up with an agency that has real-time job listings.
- Use the Staff Relief app to get instant alerts when new shifts are posted.
- Be proactive—per diem openings often fill quickly.
Whether you want the best remote nursing jobs for RNs, the stability of contract work, or the variety of per diem assignments, 2025 is the perfect year to take control of your career.
At Staff Relief, we make it easy to:
- Access the highest paying travel nursing companies
- Compare contracts side by side
- Read verified nursing agency reviews
- Secure opportunities in radiology, imaging, and allied health
- Apply once and explore thousands of jobs nationwide
Connect with Staff Relief today, and let’s build your path forward together.

Everything You Need to Know About Travel Nurse Credentialing
Every hospital, clinic, and long-term care facility has its own standards for verifying a clinician’s qualifications and readiness to practice. Even if you’ve worked at a similar facility before, you can’t automatically carry over your credentials. Each assignment requires you to complete a credentialing and onboarding process to ensure patient safety and compliance with regulations.
Credentialing typically includes:
- Drug screening
- Health assessments
- Proof of licensure and certifications
- Background checks and reference verifications
- Competency exams
- Facility-specific training and onboarding
Many nurse managers or department leaders will schedule a phone or video call to review workflows, discuss expectations, and confirm you’ve completed all requirements before your start date.
Preparation is key. Keeping all your essential documents organized will save you time and stress whenever you accept a new assignment. Here’s what you’ll need to have ready:
- Copies of your professional license(s) and any specialty certifications (such as BLS, ACLS, PALS)
- Two valid forms of identification (e.g., driver’s license and passport)
- A record of your annual physical exam (valid for one year)
- TB test results (valid for one year)
- Drug screen results
- Immunization and titer records (MMR, Varicella, Hepatitis B, and others)
- Proof of flu vaccination (especially if starting in the fall or winter)
- COVID vaccination records if required by the facility
- Payroll forms and direct deposit information
- References and verified work history
- Competency test results (if applicable)
If you want to avoid delays, consider getting your TB test, physical, and immunizations updated while you’re applying for contracts. Staying current helps you move quickly when the right opportunity arises.
Most healthcare facilities require online assessments to verify your competency in your specialty. These assessments might include:
- Skills checklists
- Clinical scenario testing
- Electronic medical record (EMR) training modules
Once you pass these evaluations, you’ll typically complete one to two days of orientation to get familiar with the facility’s policies, documentation standards, and workflows. This process helps ensure you can provide safe, effective care from day one.
If you work in in-demand roles such as ER RN, PCU RN, CT Technologist, RRT, Surgical Tech, Mammo Tech, Home Health RN, or M/S RN, expect additional verifications and specialty-specific assessments. Facilities often have strict guidelines for these positions due to the complexity of care and the need for current certifications.
Staff Relief’s credentialing team can walk you through these specialty requirements step by step so you feel confident and prepared.
Large national agencies often have more rigid, self-directed credentialing processes. Working with a regional partner like Staff Relief provides you with hands-on support. Our team will:
- Help you track deadlines for documents and assessments
- Coordinate background checks and health screenings
- Connect you with local resources for TB testing and physicals
- Answer your questions about compliance and onboarding
This personal guidance ensures nothing falls through the cracks—and you’re always ready to step into your next assignment.
Credentialing isn’t a one-time process. Here are a few habits that can help you stay organized:
- Keep a digital folder with scanned copies of your documents
- Mark your calendar with expiration dates for your TB test, physical, and certifications
- Get your annual flu shot early if you expect to start an assignment in the fall
- Check whether your next facility requires a COVID vaccine or booster
- Keep your immunizations up to date to avoid delays
Being proactive makes you more competitive for premium travel contracts and quick-start assignments.
Navigating credentialing can feel like a lot to manage, especially if you’re juggling multiple offers. That’s why choosing the right staffing partner is so important.
Staff Relief has years of experience supporting clinicians across Georgia, Alabama, Florida, and the Carolinas. Whether you’re a first-time traveler or a seasoned professional, you’ll have a dedicated team behind you to make credentialing smooth, transparent, and stress-free.
If you’re exploring travel nursing jobs or allied health contracts in the Southeast, our team is here to help you navigate credentialing and start your next adventure with confidence. Contact Staff Relief today to learn about current opportunities and get expert support every step of the way.

Addressing Georgia’s Critical Nursing Shortage
The nursing shortage in Georgia has reached critical levels in 2025, with nearly every county—urban and rural—struggling to recruit and retain qualified healthcare professionals. This crisis isn’t just about open positions; it’s about ensuring patients receive safe, timely, and compassionate care when they need it most.
From major hospitals to long-term care facilities, healthcare organizations are urgently seeking skilled nurses, surgical techs, and allied health professionals who can step into high-demand roles and make an impact.
Several factors continue to drive Georgia’s nursing shortage:
- Rising demand for healthcare services: The state’s aging population and expanded access to care have increased the need for RNs, LPNs, and allied health professionals.
- Burnout and workforce attrition: The lingering effects of the pandemic, combined with long hours and emotional stress, are pushing many clinicians to reduce hours, retire early, or leave the field altogether.
- Education and training bottlenecks: Limited capacity in nursing schools and faculty shortages continue to constrain the pipeline of new graduates.
- Rural disparities: Non-metro counties face even steeper challenges recruiting clinicians, leaving communities with limited access to primary and specialty care.
As a result, many hospitals and clinics are leaning heavily on travel contracts, per diem staff, and flexible assignments to keep up with patient needs.
The staffing shortage has ripple effects throughout Georgia’s healthcare infrastructure:
- Hospitals are relying on travel clinicians—especially in specialties like ER RNs, PCU RNs, and Surgical Techs—to fill critical gaps.
- Skilled professionals such as CT Technologists, RRTs, Mammo Techs, and Home Health RNs remain in high demand, driving up competition and pay rates.
- Burnout among the remaining workforce leads to higher turnover, further deepening shortages.
- Patients experience longer wait times, delayed procedures, and uneven access to care, particularly in rural and underserved areas.
The result is a cycle of strain that requires strategic intervention.
While the challenges are significant, Georgia’s healthcare leaders are adopting innovative strategies to rebuild the workforce and improve retention:
1. Expanding Educational Pathways
- New state investments in nursing schools and allied health programs are increasing enrollment capacity.
- Fast-track bridge programs are helping LPNs and paramedics advance to RN licensure more efficiently.
2. Financial Incentives and Career Support
- Loan repayment and tuition reimbursement programs are helping attract graduates to high-need areas.
- Retention bonuses and flexible scheduling are becoming standard in many contracts.
3. Investing in Burnout Prevention
- More facilities are offering mental health resources and dedicated time off to protect clinician well-being.
- AI-supported scheduling tools are helping balance workloads and reduce last-minute staffing gaps.
4. Expanding Telehealth and Remote Care
- Telehealth adoption continues to grow in 2025, allowing clinicians to manage certain care remotely.
- Hybrid care models are easing staffing pressures in rural counties.
5. Embracing Flexible Staffing Models
- Short-term contracts, rapid response assignments, and per diem shifts give clinicians more options to work on their terms.
- Many clinicians are finding that a mix of travel and local assignments offers better work-life balance.
Healthcare facilities across Georgia and the Southeast increasingly rely on experienced staffing agencies to fill urgent and specialized positions. When you partner with a staffing agency that understands the local landscape, you gain access to:
- Skilled clinicians ready to step into critical roles—whether it’s an ER RN, PCU RN, CT Tech, RRT, or Mammo Tech.
- Flexible workforce solutions to manage seasonal demand and unexpected absences.
- Streamlined credentialing and onboarding to get staff in place faster.
- Insights into regional pay trends and incentives.
Staff Relief, for example, has built long-standing partnerships with hospitals, outpatient centers, and home health agencies across Georgia, Florida, Alabama, and the Carolinas, making it easier to adapt to changing needs.
If you’re considering your next step in nursing or allied health, there has never been a better time to explore opportunities in Georgia. Clinicians with experience in specialties like emergency nursing, progressive care, surgical services, medical-surgical units, and diagnostic imaging are in especially high demand.
With flexible contracts, competitive compensation, and support from experienced recruiters, you can build a career that aligns with your goals and helps meet a pressing need.
Georgia’s nursing shortage is a complex, urgent issue—but progress is happening. By investing in education, supporting the workforce, embracing innovation, and building strong partnerships, the state is working to rebuild its healthcare capacity.
If you’re a healthcare professional ready to make an impact—or a facility seeking experienced clinicians—this is the moment to take action.
Ready to explore the latest opportunities or learn how strategic staffing can help? Contact Staff Relief today and join the effort to strengthen Georgia’s healthcare system for everyone.

10 Tips for Travel Nurses
Travel healthcare is more than just an assignment, it’s an opportunity to expand your skills, explore new places, and make an impact where it matters most. Whether you’re a seasoned travel nurse, a respiratory therapist, or a surgical technologist, knowing how to navigate contracts and maximize your experience is key to success.
Here are ten essential tips every travel healthcare professional should keep in mind.
1. The Demand for Your Skills is Higher Than Ever
In 2025, healthcare facilities across the Southeast in Georgia, Alabama, Florida, and the Carolinas are experiencing critical staffing shortages. High-demand specialties like CT Tech, ER RN, Surgical Tech, RRT, PCU RN, Mammo Tech, Home Health RN, and M/S RN are seeing unprecedented opportunities.
Travel nursing jobs and allied health contracts are plentiful, but competition can be fierce for the best assignments. Staying flexible and proactive will help you secure roles that match your expertise and goals.
2. Understand Tax Implications of Travel Assignments
Many clinicians overlook how travel pay affects their taxes. Housing stipends, travel reimbursements, and per diem allowances can all impact your taxable income. It’s wise to consult a tax professional who understands healthcare contracts to ensure you’re planning ahead and taking advantage of eligible deductions.
3. Credentialing and Compliance Take Preparation
Every state has different licensure and credentialing requirements. Georgia, Florida, and the Carolinas all have their own rules around background checks and health records.
Be prepared to provide:
- A TB test (valid for 1 year)
- A current physical exam (valid for 1 year)
- Titers and immunization records
- A background check
- A drug screen
It’s smart to get your TB test, physical, and immunizations done while you’re applying so you’re ready as soon as you receive an offer. Keep your immunizations updated, including your flu shot in the fall and COVID vaccinations where required. This will prevent delays when it’s time to start your contract.
Working with a healthcare staffing agency like Staff Relief ensures you’ll have help coordinating these documents and understanding what’s required for each facility.
4. Housing Options Vary by Assignment
Some contracts include housing stipends, while others offer pre-arranged accommodations. It’s critical to understand:
- What your stipend covers
- Whether you’ll be responsible for utilities, deposits, or furniture
- How your housing affects your taxable income
If you prefer to find your own place, Staff Relief can help source local housing options and connect you to reputable providers in your assignment area.
5. Your Reputation Will Follow You
Healthcare facilities often work with the same staffing partners across regions. Showing up on time, being adaptable, and maintaining professionalism will build your reputation and make it easier to secure future assignments.
Positive references can help you access competitive roles in specialties like ER, PCU, and surgical services.
6. Flexibility is Your Superpower
The most successful travel clinicians are those who can pivot quickly. Being open to night shifts, rural contracts, or high-demand specialties often results in higher pay and priority placement.
If you’re willing to work in critical areas, you’ll find more opportunities and stronger negotiating power.
7. Pay Packages Can Be Complex
Your compensation may include:
- Base hourly pay
- Travel stipends
- Housing allowances
- Completion bonuses
Make sure you understand the full picture, not just the hourly rate. This is essential so that you can budget effectively. A reputable healthcare staffing agency will always be transparent about how your pay is structured.
8. Burnout is Real so Take Care of Yourself
Long shifts and adapting to new teams can be stressful. Protect your mental health by:
- Scheduling regular downtime between contracts
- Accessing telehealth services offered through Staff Relief for confidential support
- Staying connected to your support network
Prioritizing self-care helps you bring your best to every assignment.
9. Smaller Agencies Can Get You Into Hidden-Gem Facilities
Smaller agencies can often place clinicians into smaller community hospitals and rural facilities where patient loads are more manageable, but pay rates remain competitive. These positions are available through Staff Relief in Georgia, Alabama, and South Carolina. Only Staff Relief and one or two other boutique firms serve these facilities, so you won’t find these assignments through large national agencies like Aya, Medical Solutions, or AMN Healthcare.
10. Choosing the Right Staffing Partner Matters
Your agency isn’t just your employer, it’s your advocate. The best healthcare staffing partners:
- Have deep relationships with respected hospitals and clinics
- Offer personal support before, during, and after your assignment
Staff Relief has decades of experience supporting clinicians across the Southeast, combining local expertise with a commitment to transparency and respect.
If you’re exploring travel nursing jobs or allied health contracts in Georgia and beyond, now is the time to take the next step. With the right support and preparation, your travel career can be rewarding, sustainable, and full of growth. Contact Staff Relief today to learn about current opportunities and find the right fit for your skills and goals.

How to Choosing the Right Medical Staffing Agency
Choosing the right medical staffing agency isn’t just about finding a job—it’s about building a career with the support, transparency, and opportunities you deserve. Whether you’re looking for contract nursing jobs, travel assignments, or allied health positions, partnering with the right agency helps you feel confident every step of the way.
As a regional leader in the Southeast serving Georgia, the Carolinas, Alabama, and Florida, Staff Relief specializes in high-demand roles and offers deep local expertise to help you succeed.
Here are six essential tips to guide your search for a medical staffing agency you can trust.
1. Work with a Partner Who Knows the Region
When you’re working in states across the Southeast, you want an agency that understands the unique dynamics of each market. Regional experience matters because:
- Different states have varying credentialing and compliance requirements
- Compensation rates shift between urban and rural facilities
- Each area has its own demand for specialties, including CT Tech, ER RN, Surgical Tech, RRT, PCU RN, Mammo Tech, Home Health RN, and M/S RN assignments
Staff Relief’s recruiters have years of experience placing clinicians throughout Georgia, Alabama, Florida, and the Carolinas. This local knowledge ensures you’re matched with facilities that fit your skills, preferences, and professional goals.
2. Evaluate the Agency’s Reputation and Track Record
A medical staffing agency’s history is a strong indicator of what you can expect. Take time to:
- Explore the agency’s website to see testimonials from nurses, surgical techs, respiratory therapists, and imaging professionals
- Review social media and online platforms for authentic feedback
- Look for examples of long-term partnerships with respected hospitals, outpatient centers, and home health organizations across the Southeast
When you choose an agency that has established relationships and a reputation for consistency, you gain peace of mind that your career is in capable hands.
3. Expect Clear Communication About Pay
Transparency around compensation is crucial. Medical staffing pay packages can include:
- Base hourly rates
- Travel and housing stipends
- Bonuses
Without clarity, it’s easy to feel uncertain about what you’ll actually earn. A trustworthy agency will explain exactly how your pay is structured, whether you’re taking on a rapid response ER RN contract, a CT Tech travel assignment, or a Mammo Tech position.
At Staff Relief, we prioritize transparent communication so you can make informed decisions and feel confident in your earnings.
4. Assess Benefits and Support
The right staffing agency offers more than just placements. Look for a partner that provides:
- Credentialing and compliance support
- Guidance navigating state requirements if you’re crossing from Georgia into Florida, Alabama, or the Carolinas
- Professional development resources and scheduling assistance
Staff Relief is committed to offering comprehensive support, so you can focus on providing excellent patient care, whether you’re working in PCU, ER, surgical services, or home health.
5. Look for Joint Commission Certification
When an agency is Health Care Staffing certified by The Joint Commission, it demonstrates a commitment to quality and safety. Certification means the agency has:
- Passed rigorous evaluations of processes, compliance, and clinical standards
- Demonstrated consistent excellence in recruiting and supporting healthcare professionals
This recognition shows you’re working with an organization that meets the highest standards. This is something you can expect when partnering with Staff Relief.
6. Find the Right Fit for Your Working Style
Every agency operates differently. Some rely on automated platforms and self-service tools, while others offer more personal, one-on-one support.
Ask yourself:
- Do you want direct access to a recruiter who knows you by name?
- Would you rather work with an agency that manages credentialing and logistics for you?
- Do you prefer a more high-touch approach over an impersonal online process?
Choosing an agency that fits your communication style and values makes every assignment more rewarding. Staff Relief’s approach is personal, responsive, and focused on helping you thrive in the role that’s right for you.
When you work in specialized, high-demand fields like CT Tech, ER RN, Surgical Tech, RRT, Mammo Tech, PCU RN, Home Health RN, and M/S RN. You deserve a staffing partner who understands your expertise and advocates for your success.
The right agency combines:
- Regional knowledge of healthcare employers throughout Georgia, Alabama, Florida, and the Carolinas
- Transparent, competitive pay structures
- Robust support and credentialing assistance
- A proven reputation with hospitals and clinics across the Southeast
- Certification that demonstrates credibility
- A commitment to personal service and professional respect
With the right support you’re not just taking a job, you’re building a sustainable career.
If you’re exploring your next contract or travel assignment in the Southeast, Staff Relief is here to help. Our partnerships with respected healthcare facilities and our experience placing clinicians in high-demand specialties mean you can feel confident you’re making the best move for your future.
Contact us today to learn more about available positions and start your search with a staffing agency that puts you first.


The Cost of Nurse Turnover: A Breakdown
Poor nurse retention is a major issue for healthcare facilities, with the national registered nurse (RN) turnover rate standing at nearly 20%. According to the 2024 NSI National Healthcare Retention and RN Staffing Report, the average cost of nurse turnover is estimated to be $56,300 per every RN who leaves their job. For the average hospital, this can equate to roughly $3.9 to $5.8 million in losses per year.
Beyond the financial impacts, high turnover can also have rippling effects on company culture and patient care. In this article, we’ll break down all the costs of nurse turnover and outline strategies that can help you mitigate this issue at your facility.
Nurse turnover occurs when nursing professionals leave their jobs or the profession altogether. This can include instances in which staff are involuntarily terminated from their positions, enter retirement, or choose to leave their roles for other reasons. Some of the most common reasons why nursing professionals willingly leave their jobs include burnout, feeling underappreciated, and a lack of peer support.
Before we break down the cost of nursing turnover, it’s important to note that national nurse turnover and cost estimates often only account for RNs. While it’s difficult to estimate a turnover rate that is representative of all levels of nursing, let’s take a look at how turnover rates and costs have been reported for other types of roles:
- The cost of nurse practitioner turnover is estimated to be $85,832 to $114,919 per episode, with the average turnover rate standing at roughly 10%.
- The cost of nurse managerturnover is estimated to be between $132,00 to $228,000 per episode, with some hospitals reporting that 50% of their nurse leaders intend to leave their jobs within 5 years.
- The indirect costs of replacing one certified nursing assistant (CNA) can range from $3,000 to $6,000, with turnover rates averaging as high as 50% in nursing homes alone.
From these statistics, it’s clear that turnover costs can add up quickly if nursing professionals keep leaving their positions. But how exactly does turnover amount to millions of dollars per year? Here’s a rundown of what can contribute to both the economic and non-economic costs.
There are several ways in which frequent turnover can lead to increased operational costs for facilities. We’ll review and summarize these costs below.
Costs of Vacancies
When a nurse leaves their position, facilities must spend excess money to compensate for vacancies and understaffing. This includes the costs of advertising the opening, hiring temporary staff, and paying existing staff for overtime. Facilities may even need to close beds and defer patients, which leads to diminishing returns.
Several studies have found that these factors combined can contribute to significant losses, accounting for anywhere between 44% to 83% of turnover costs. These costs also continue to rise the longer a position stays open.
Costs of Training
Each time a facility hires a new nurse, additional resources must be spent for onboarding and training. Research has suggested that training can account for roughly 7% to 9% of turnover costs, as preceptors are often given temporary salary raises to orient new nurses.
Facilities that invest in new nurse residency programs are also estimated to incur an additional training cost of roughly $2,041 per resident. Residency programs are often used as a strategy to improve new nurse retention. But if turnover remains high for other reasons, these programs can have a lower return on investment.
Costs of Productivity Loss
Studies have also shown that initial reductions in productivity can contribute to a large proportion of losses, accounting for roughly 45% to 88% of turnover costs. This is because facilities are essentially paying two nurses to do the work of one during training periods — with some preceptorships lasting months at a time.
Additionally, there can be variations in skill level when facilities use a mix of temporary staff. This means that managers may need to spend more time overseeing care, which also contributes to reduced productivity at the leadership level.
High turnover can also impact the overall workflow and culture at a facility. These non-economic costs are important to consider since they can, conversely, lead to more turnover and create a cyclical issue over time.
Poor Teamwork
High turnover means that the entire nursing team must frequently adapt to new personalities and workstyles. Studies have shown that this can worsen communication and collaboration, impacting the overall cohesiveness of the unit. This can also make it more difficult to retain new hires, since teams may come across as unsupportive.
Lower Quality of Care
When existing staff take on increased workloads to compensate for gaps in staffing, quality of care can go down. Some studies have even shown that high turnover can significantly increase the rate of medical errors, mortality, pressure ulcers, and length of stay.
Reduced Employee Morale
The fragmented communication and increased stress resulting from high turnover can also lower staff morale. This may contribute to burnout, which can cause even more nurses to leave their jobs if staff retention and job satisfaction aren’t made a priority.
While there are many different causes of nurse turnover, studies have shown that nurses are four times more likely to voluntarily leave their positions than to get involuntarily terminated. This means that comprehensive measures at the institutional level are needed to retain staff and keep them satisfied in their roles.
Fundamentally, it’s important to engage your staff in conversations and identify the root causes of turnover at your facility. From there, you can apply more meaningful solutions that help your staff feel supported. This may include:
- Using sustainable staffing alternatives that allow for manageable workloads.
- Empowering nurses by giving them more control over their schedules and work.
- Creating a healthy work environment to prevent staff burnout.
- Providing transparent, consistent, and objective leadership.
The cost of nurse turnover can impact the operations, care quality, and culture at your facility. Need solutions that will stabilize your workforce in the long run? Get dozens of free, expert-written facility management tips and insights delivered straight to your inbox.
https://www.intelycare.com/facilities/resources/the-cost-of-nurse-turnover-a-breakdown/
KPMG’s 2017 U.S. Hospital Nursing: Labor Costs Study
This study identifies several trends and benchmarks in relation to hospital nursing labor costs in the United States. Some of the key findings are summarized below. When all costs are considered, traveling nurses appear to cost less than permanent nurses on an hourly basis. Cost data provided by hospitals indicates that the hourly, all-in cost for a full-time, permanent nurse is approximately $89. This hourly cost is higher than traveling nurses that cost approximately $83 per hour. Key costs that are after captured in this all-in measure are overtime pay, paid time off, retirement, insurance, recruiting, and payroll taxes – and these costs vary by nurse type. Additionally, the survey finds a quantifiable “hidden” cost associated with permanent nurses that is the result of non-productive labor hours, and an unquantified “hidden” cost associated with attrition and time required to fill a permanent direct care registered nurse position. Respondents to the survey indicated that traveling nurses are widely used today, representing approximately 11 % of respondent’s nursing staffs. Also, these hospitals indicated their use of traveling nurses will likely continue to grow in the future. Primary factors for this upward trend are local nursing shortages and facility growth. In all, traveling nurses appear to be a cost effective source of labor tor hospitals, and hospitals are forecasting higher usage of these nurses in the future.

2025 NSI National Health Care Retention & RN Staffing Report
With people living longer, the subsequent rise in chronic conditions and the fact that all Baby Boomers will reach retirement age by 2030, recruiting and retaining quality staff will continue to be a top healthcare issue for years to come. Last year, hospitals increased staff by adding ~304,000 employees, a 5.4% add rate. Of this, ~98,000 RNs were hired which represents a 5.6% RN add rate.
Hospital and RN turnover continue to fall but both remain slightly elevated. Nationally, the hospital turnover rate stands at 18.3%, a 2.4% decrease from CY23, and RN turnover is recorded at 16.4%, a 2.0% decrease. Registered Nurses working in pediatrics, women’s health, and surgical services reported the lowest turnover rate, while nurses working in behavior health, step down and emergency services experienced the highest.
The cost of turnover can have a profound impact on diminishing hospital margins and needs to be managed. According to the survey, the average cost of turnover for a bedside RN is $61,110, an 8.6% increase, resulting in the average hospital losing between $3.9m – $5.7m. Each percent change in RN turnover will cost/save the average hospital an additional $289,000/yr.
The RN vacancy rate also remains elevated at 9.6% nationally. While 0.3% lower than last year, over forty percent (41.8%) reported a vacancy rate of ten percent or more. The RN Recruitment Difficulty Index decreased three (3) days to an average of 83 days. In essence, it takes approximately 3 months to recruit an experienced RN, with step down and med/surg presenting the greatest challenges. Feeling financial stress, hospitals will continue to focus on controlling the high cost of labor with contract labor being a top strategy to navigate a staffing shortage. The greatest potential to offset margin compression is in the top budget line item (labor expense). Every RN hired saves $79,100. An NSI contract to replace 20 travel nurses could save your institution $1,582,000.
2024 Employer Health Benefits Survey
Employer-sponsored insurance covers 154 million nonelderly people. To provide a current snapshot of employer sponsored health benefits, KFF conducts an annual survey of private and non-federal public employers with three or more workers. This is the 26th Employer Health Benefits Survey (EHBS) and reflects employer-sponsored health benefits in 2024.
Hiring More Nurses Generates Revenue for Hospitals
Underfunding is driving an acute shortage of trained nurses in hospitals and care facilities in the United States. It is the worst such shortage in more than four decades. One estimate from the American Hospital Association puts the deficit north of one million. Meanwhile, a recent survey by recruitment specialist AMN Healthcare suggests that 900,000 more nurses will drop out of the workforce by 2027.
American nurses are quitting in droves, thanks to low pay and burnout as understaffing increases individual workload. This is bad news for patient outcomes. Nurses are estimated to have eight times more routine contact with patients than physicians. They shoulder the bulk of all responsibility in terms of diagnostic data collection, treatment plans, and clinical reporting. As a result, understaffing is linked to a slew of serious problems, among them increased wait times for patients in care, post-operative infections, readmission rates, and patient mortality—all of which are on the rise across the U.S.
Tackling this crisis is challenging because of how nursing services are reimbursed. Most hospitals operate a payment system where services are paid for separately. Physician services are billed as separate line items, making them a revenue generator for the hospitals that employ them. But under Medicare, nursing services are charged as part of a fixed room and board fee, meaning that hospitals charge the same fee regardless of how many nurses are employed in the patient’s care. In this model, nurses end up on the other side of hospitals’ balance sheets: a labor expense rather than a source of income.
For beleaguered administrators looking to sustain quality of care while minimizing costs (and maximizing profits), hiring and retaining nursing staff has arguably become something of a zero-sum game in the U.S.
But might the balance sheet in fact be skewed in some way? Could there be potential financial losses attached to nurse understaffing that administrators should factor into their hiring and remuneration decisions?
Research by Goizueta Professors Diwas KC and Donald Lee, as well as recent Goizueta PhD graduates Hao Ding 24PhD (Auburn University) and Sokol Tushe 23PhD (Muma College of Business), would suggest there are. Their new peer-reviewed publication* finds that increasing a single nurse’s workload by just one patient creates a 17% service slowdown for all other patients under that nurse’s care. Looking at the data another way, having one additional nurse on duty during the busiest shift (typically between 7am and 7pm) speeds up emergency department work and frees up capacity to treat more patients such that hospitals could be looking at a major increase in revenue. The researchers calculate that this productivity gain could equate to a net increase of $470,000 per 10,000 patient visits—and savings to the tune of $160,000 in lost earnings for the same number of patients as wait times are reduced.
“A lot of the debate around nursing in the U.S. has focused on the loss of quality in care, which is hugely important,” says Diwas KC.
But looking at the crisis through a productivity lens means we’re also able to understand the very real economic value that nurses bring too: the revenue increases that come with capacity gains.Diwas KC, Goizueta Foundation Term Professor of Information Systems & Operations Management
“Our findings challenge the predominant thinking around nursing as a cost,” adds Lee. “What we see is that investing in nursing staff more than pays for itself in downstream financial benefits for hospitals. It is effectively a win-win-win for patients, nurses, and healthcare providers.”
To get to these findings, the researchers analyzed a high-resolution dataset on patient flow through a large U.S. teaching hospital. They looked at the real-time workloads of physicians and nurses working in the emergency department between April 2018 and March 2019, factoring in variables such as patient demographics and severity of complaint or illness. Tracking patients from admission to triage and on to treatment, the researchers were able to tease out the impact that the number of nurses and physicians on duty had on patient throughput. Using a novel machine learning technique developed at Goizueta by Lee, they were able to identify the effect of increasing or reducing the workforce. The contrast between physicians and nursing staff is stark, says Tushe.
“When you have fewer nurses on duty, capacity and patient throughput drops by an order of magnitude—far, far more than when reducing the number of doctors. Our results show that for every additional patient the nurse is responsible for, service speed falls by 17%. That compares to just 1.4% if you add one patient to the workload of an attending physician. In other words, nurses’ impact on productivity in the emergency department is more than eight times greater.”
Adding an additional nurse to the workforce, on the other hand, increases capacity appreciably. And as more patients are treated faster, hospitals can expect a concomitant uptick in revenue, says KC.
“It’s well documented that cutting down wait time equates to more patients treated and more income. Previous research shows that reducing service time by 15 minutes per 30,000 patient visits translates to $1.4 million in extra revenue for a hospital.”
In our study, we calculate that staffing one additional nurse in the 7am to 7pm emergency department shift reduces wait time by 23 minutes, so hospitals could be looking at an increase of $2.33 million per year.Diwas KC
This far eclipses the costs associated with hiring one additional nurse, says Lee.
“According to 2022 U.S. Bureau of Labor Statistics, the average nursing salary in the U.S. is $83,000. Fringe benefits account for an additional 50% of the base salary. The total cost of adding one nurse during the 7am to 7pm shift is $310,000 (for 2.5 full-time employees). When you do the math, it is clear. The net hospital gain is $2 million for the hospital in our study. Or $470,000 per 10,000 patient visits.”
These findings should provide compelling food for thought both to healthcare administrators and U.S. policymakers. For too long, the latter have fixated on the upstream costs, without exploring the downstream benefits of nursing services, say the researchers. Their study, the first to quantify the economic value of nurses in the U.S., asks “better questions,” argues Tushe; exploiting newly available data and analytics to reveal incontrovertible financial benefits that attach to hiring—and compensating—more nurses in American hospitals.
We know that a lot of nurses are leaving the profession not just because of cuts and burnout, but also because of lower pay. We would say to administrators struggling to hire talented nurses to review current wage offers, because our analysis suggests that the economic surplus from hiring more nurses could be readily applied to retention pay rises also.Sokol Tushe 23PhD, Muma College of Business
For state-level decision makers, Lee has additional words of advice.
“In 2004, California mandated minimum nurse-to-patient ratios in hospitals. Since then, six more states have added some form of minimum ratio requirement. The evidence is that this has been beneficial to patient outcomes and nurse job satisfaction. Our research now adds an economic dimension to the list of benefits as well. Ipso facto, policymakers ought to consider wider adoption of minimum nurse-to-patient ratios.”
However, decision makers go about tackling the shortage of nurses in the U.S., they should go about it fast and soon, says KC.
“This is a healthcare crisis that is only set to become more acute in the near future. As our demographics shift and our population starts again out, demand for quality will increase. So too must the supply of care capacity. But what we are seeing is the nursing staffing situation in the U.S. moving in the opposite direction. All of this is manifesting in the emergency department. That’s where wait times are getting longer, mistakes are being made, and overworked nurses are quitting. It is creating a vicious cycle that needs to be broken.”
Goizueta faculty apply their expertise and knowledge to solving problems that society—and the world—face. Learn more about faculty research at Goizueta.
*Ding, Tushe, Kc, Lee: “Frontiers in Operations: Valuing nursing productivity in emergency departments.” Manufacturing & Service Operations Management 26:4:1323-1337 (2024)
Georgia could see the largest shortage of RNs by 2036
Staffing is one of the biggest issues facing ASCs. A 2023 survey from ORManager found that in the last 12 months, 56% of ASCs reported an increase in volume. Despite this success, 68% of facilities also reported having a more difficult time recruiting experienced operating room nurses.
“I think the biggest threat towards ASCs in 2023 is staffing, especially qualified, experienced staffing in all areas of an ASC, including business office, pre-op, OR (both nursing and surgical technicians), post-anesthesia care unit and recovery nurses. In addition, sterile processing technicians,” Michael Powers, administrator of Knoxville, Tenn.-based Children’s West Surgery Center, told Becker’s. “Each of these areas require a certain set of skills that are acquired and honed over time. There is increased competition, and in fact it is hard to compete with large health systems/hospitals. I am also finding that ASCs are competing in the same region against one another for the available staffing pool.”
The HRSA report highlights nurse workforce projections from 2021 to 2036 generated using the agency’s health workforce simulation.
Here are the five states with the largest projected shortages of registered nurses by 2036, per the report:
1. Georgia: 29% projected shortage
Projected vacancies: 34,800
2. California: 26% projected shortage
Projected vacancies: 106,310
3. Washington: 26% projected shortage
Projected vacancies: 22,700
4. New Jersey: 25% projected shortage
Projected vacancies: 24,450
5. North Carolina: 23% projected shortage
Projected vacancies: 31,350
https://www.beckersasc.com/leadership/5-states-facing-the-biggest-nurse-shortages-by-2036

Nursing Shortage Fact Sheet
The U.S. is projected to experience a shortage of Registered Nurses (RNs) that is expected to intensify as Baby Boomers age and the need for health care grows. Compounding the problem is the fact that nursing schools across the country are struggling to expand capacity to meet the rising demand for care. The American Association of Colleges of Nursing (AACN) is working with schools, policy makers, nursing organizations, and the media to bring attention to this healthcare concern. AACN is leveraging its resources to shape legislation, identify strategies, and form collaborations to address the shortage.
For more information including below, see attached PDF:
- Current and Projected Shortage Indicators
- Contributing Factors Impacting the Nursing Shortage
- Impact of Nurse Staffing on Patient Care
- Efforts to Address the Nursing Shortage
The cost of nurse turnover in 24 numbers
The 2024 NSI National Health Care Retention & RN Staffing Report features input from 400 hospitals in 36 states on registered nurse turnover, retention, vacancy rates, recruitment metrics and staffing strategies.
It found the average cost of turnover for one staff RN grew from January through December 2023 to $56,300, among other dollar figures and statistics that are helpful to understand the financial implications of one of healthcare’s most challenging labor disruptions.
Here are 24 numbers that illustrate the cost of nurse turnover, according to the most recent edition of the report, which is available in full here.
1. The turnover rate for staff RNs decreased by 4.6% in 2023, resulting in a national average of 18.4%. Given varying bed size, RN turnover can range from 5.6% to 38.8%.
2. The average cost of turnover for a staff RN increased by 7.5% in the past year to $56,300, with a range of $45,100 to $67,500. This is up from the average cost of turnover for an RN in 2022, which was $52,350.
3. Each percent change in RN turnover stands to cost or save the average hospital $262,500 per year.
4. The RN vacancy rate sits at 9.9% nationally. This marks an improvement, as hospitals hired an additional 153,000 RNs in 2023 and lowered the vacancy rate by 5.8%.
5. The average time to recruit an experienced RN ranges from 59 to 109 days, with the average for 2023 sitting at 86 days — nine days quicker than the year prior.
7. Every region represented in the 2024 report recorded a decrease to RN turnover, ranging from -1% to -5.1%. The South Central region saw the high end of this range while the North Central region saw the low end.
8. Over the past five years, RNs in step down, emergency services, and telemetry were most mobile with a cumulative turnover rate between 112% and 119%. “Essentially, these departments will turn over their entire RN staff in less than four and a half years,” the report states.
9. RNs in pediatrics, surgical services, and women’s health were less mobile, with 2023 turnover rates of 13.3%, 15.4% and 16.3%, respectively.
https://www.beckershospitalreview.com/finance/the-cost-of-nurse-turnover-in-24-numbers-2024
Costs and cost-effectiveness of improved nurse staffing levels and skill mix in acute hospitals
Extensive research shows associations between increased nurse staffing levels, skill mix and patient outcomes. However, showing that improved staffing levels are linked to improved outcomes is not sufficient to provide a case for increasing them. This review of economic studies in acute hospitals aims to identify costs and consequences associated with different nurse staffing configurations in hospitals.
Although more evidence on cost-effectiveness is still needed, increases in absolute or relative numbers of registered nurses in general medical and surgical wards have the potential to be highly cost-effective. The preponderance of the evidence suggests that increasing the proportion of registered nurses is associated with improved outcomes and, potentially, reduced net cost. Conversely, policies that lead to a reduction in the proportion of registered nurses in nursing teams could give worse outcomes at increased costs and there is no evidence that such approaches are cost-effective. In an era of registered nurse scarcity, these results favour investment in registered nurse supply as opposed to using lesser qualified staff as substitutes, especially where baseline nurse staffing and skill mix are low.
https://www.sciencedirect.com/science/article/pii/S0020748923001669
American Hospital Association Health Care Workforce Scan
The pandemic exacerbated existing shortages of health care workers in all roles, from clinicians to environmental and food services to admissions and scheduling. These shortages will persist well beyond the pandemic given today’s highly competitive labor market.
Record numbers of people are leaving their current jobs for new ones, new fields or new pursuits outside the job market altogether.
Despite all the difficulties, trauma and challenges they have faced, millions continue to show up and believe in their ability to make a difference in patients’ lives. Their mental and physical well-being requires tangible help and support from their leaders, and respect from the communities they serve.
The incredible challenges have also created unique opportunities to accelerate change and improve the way care is delivered, whether through technology, new care delivery approaches or multidisciplinary team models.
Ensuring the health and safety of the health care workforce – and the health and safety of the patients they care for – requires commitment at the individual, organizational and community level.

The Real Costs of Healthcare Staff Turnover
Staffing tops the list of healthcare industry challenges heading into 2023, according to polling data from healthcare advocacy group MGMA. It’s no wonder: Hospital staff turnover rates climbed as high as 26% in 2021 as workers retired due to burnout or went to work for organizations offering higher pay or better work-life balance.
For healthcare organizations, high employee turnover rates are a burden on finances and resources. Turnover costs include the expense of recruiting, hiring, and training new employees, as well as the cost of temporarily filling staffing gaps with expensive contract workers. There’s also the cost of reduced productivity as managers shift much of their attention to hiring and as new hires get up to speed. A less tangible—but still significant—turnover cost is lower employee morale as those who remain work harder to fill gaps for less pay than contract workers hired to provide temporary coverage.
Employee turnover refers to the total number of workers who leave a company over a specific period of time. Companies measure involuntary departures (layoffs and firings) and voluntary turnover (resignations) as well as the cost of replacing a given type of employee. Considering turnover can provide opportunities to replace underperformers, many employers also calculate the ideal turnover rate for their organization so managers can set specific employee retention goals. Every company has employee turnover—farsighted companies take the time to understand their turnover rate, the factors driving turnover, and what they can do to build and retain a workforce that will help achieve their organizational goals.
Key Takeaways
- Even before COVID-19, more than half of doctors and nurses reported symptoms of burnout, defined by physical and/or emotional exhaustion due to the rigors of the profession. But the pandemic shifted burnout into overdrive. During the pandemic, 93% of health workers reported experiencing stress.
- The average cost of turnover for a regular position is between six and nine months of an employee’s salary. Replacing a highly specialized healthcare professional can cost as much as 200% of the employee’s yearly salary.
- Patients notice high turnover rates when they see the impact of poor patient-to-staff ratios. They lose confidence in their healthcare provider when they don’t believe they’re receiving the best care, which can cause reputational damage.
In 2022, turnover rates for segments of the healthcare industry ranged from 19.5% at hospitals to 65% for at-home care providers to 94% at nursing homes.
This level of turnover puts a huge financial and logistical burden on healthcare providers. While COVID-19 put additional stress on the healthcare labor force, and the industry will likely feel the effects of COVID for years to come, the healthcare staffing crisis existed long before the pandemic. The following factors are also contributing to today’s healthcare worker exodus:
Inflexible, demanding schedules
Healthcare jobs are notorious for long hours and erratic schedules, and many are considered “deskless” jobs, meaning workers spend much of their time on the move. In fact, it’s estimated that nurses in hospitals walk about five miles a day.
Excessive administrative work
Fictional doctors and nurses are often depicted standing by a patient’s bedside, developing personal relationships and providing hands-on care. In reality, providers no longer have sufficient time to spend one-on-one with patients and other caregivers. Instead, they’re burdened by documentation, charting, and other administrative tasks. In 2021 doctors reported spending, on average, 15.6 hours per week on paperwork and other administrative tasks. First-year medical residents spend only about 10% of their work time face-to-face with patients, according to a study from Penn Medicine and Johns Hopkins University.
Heavy workloads
Even before COVID-19, more than half of nurses and physicians reported symptoms of burnout, according to the U.S. Department of Health and Human Services, and burnout rates have worsened over the past several years due to heavy workloads and related job stress. (A person experiencing burnout suffers from emotional exhaustion, depersonalization—a sense of detachment from oneself—and a reduced sense of personal accomplishment.) During the pandemic, researchers found that 93% of health workers were experiencing stress, 86% had anxiety, and 76% reported exhaustion.
Disconnection from managers
Healthcare workers who don’t work in a single location, such as nurses, medical assistants, and respiratory therapists, may miss out on opportunities to interact with their managers in person. Cut off from these critical personal connections, they can feel underappreciated and unseen, which makes it more likely they’ll look for a job elsewhere.
Relatively low pay
Many nurses feel they aren’t getting the pay they deserve. Even with a median annual salary of US$77,600, 66% of nurses describe pay as their No. 1 consideration when planning their next career move, according to a survey by Vivian, a healthcare hiring platform.
The direct costs of high employee turnover—the costs of recruiting, onboarding, and training new people and the costs of hiring contract staff to fill empty positions—are relatively easy to measure. The indirect costs are less quantifiable but just as burdensome; they include reduced patient satisfaction and lower employee morale. Consider these costs as you assess the impact of employee turnover on your organization.
1. Separation costs
These include severance pay, costs associated with unemployment insurance claims, payments for any ongoing benefits, and the costs associated with exit interviews and removing employees from all internal systems and directories.
2. Hiring costs
Turnover costs an organization much more than money. There’s the cost of reduced productivity when an employee leaves, and the hiring process itself can be expensive and resource intensive. It costs an employer an average of between six and nine months of an employee’s annual salary to replace them, according to the Society for Human Resource Management, and it can cost as much as 200% of the employee’s annual pay to replace a specialized healthcare professional.
3. Training costs
Even highly skilled and experienced employees need time to adapt to a new job. The healthcare industry has mandatory training and certification requirements that don’t exist in other industries. Unfortunately, many healthcare employees don’t feel they’re getting the right skills training for their rapidly changing roles, and managers and healthcare HR teams struggle to track and enforce training requirements.
4. Contingent labor costs
Understaffed healthcare organizations often resort to hiring travel or contract staff to fill workforce gaps. Unfamiliar with a facility’s policies, staff, and even its geography, contract workers can reduce overall productivity and burden full-time employees.
5. Substandard patient care
High employee turnover can lead to unsafe staff-to-patient ratios that make it hard to provide the best care. With too many patients to monitor, nurses and aides can overlook issues that slow recovery times and endanger patients. A study by the US National Institutes of Health showed that patients can lose confidence in their healthcare provider when they don’t believe they’re receiving the best care, which can tarnish the provider’s reputation.
6. Lower morale
The US healthcare industry lost more than 500,000 employees each month in 2022, according to the U.S. Bureau of Labor Statistics, and those left behind are dispirited about the future. In 2021, nearly three quarters of healthcare employees surveyed by Vivian, a healthcare hiring platform, said that workplace morale had gotten worse over the previous 12 months, and only 20% said they’re optimistic about the future of healthcare in the US. This lack of employee engagement is likely to increase employee turnover rates and reduce patient care levels, negatively impacting a healthcare organization’s reputation and financial health.
To reduce healthcare staff turnover (PDF), organizations must first improve employee well-being. People want to be compensated fairly, but beyond that, they want to be surrounded by coworkers and managers they respect. They want to feel ownership of their work lives and find work-life balance. They want systems and processes that are easy to navigate so they can focus on what matters—patient care. Here are some steps healthcare organizations can take to reduce turnover.
Managers who practice intentional hiring take the time to develop a clear job description for an open role and a clear plan for finding the right set of candidates. It may feel like this preparation lengthens the hiring process, but in the long run, it will pay off for the organization and for the candidates’ coworkers.
There are complications inherent in managing any 24/7 workforce, but these complications are compounded in healthcare by the need to have people with specific education, training, and certifications present at all times. The latest cloud-based human capital management (HCM) systems give managers visibility into staffing needs and availability and allow them to anticipate and cover surges.
Giving new employees the right tools at the start allows them to get a clear sense of the organization’s training goals and how they can fit training requirements into their workday. Dashboards that show employees what training they need, and when they need it, can improve compliance numbers while showing HR staff who’s falling behind. Cloud-based HCM systems let employees set their own training pace and measure their progress, which is especially valuable in busy workplaces where staff may have limited time to devote to training.
Healthcare professionals look for organizations that offer professional development programs beyond what’s required by law, including courses in management, communications, and ethics.
The stress of logging long hours in challenging situations is compounded by having to use inflexible, out-of-date, unconnected systems. Prospect Medical Holdings, which operates 17 hospitals and 165 medical care clinics across five states, at one time had 37 different HCM systems before successfully centralizing operations on a single cloud platform. A cloud HCM system enables employees to choose flexible schedules, sends workers notifications when it’s time to take a break, and allows management to send out regular communications that make workers feel more connected to the organization.
Healthcare-specific recruiting features in Oracle Fusion Cloud HCM help hospitals and other providers attract the best doctors, nurses, physician assistants, therapists, technicians, and support staff while giving them the tools they need to retain their accreditations and grow their expertise.
Oracle Cloud HCM’s workforce management capability enables staff to manage their schedules, sign up for shifts on their mobile devices, and block off time when they’re not available—giving them the ability to manage when and where they work. Healthcare providers can also use the cloud application’s dashboards to stay informed about patient counts and resource requirements so they can make shift changes as needed. Additionally, Oracle Cloud HCM’s employee experience platform makes it easy for hospital leaders to keep employees informed about significant organizational news and initiatives and, through pulse surveys, learn about employee concerns and needs.
Technology alone will never solve the healthcare industry’s employee turnover problem. That will take concerted efforts by healthcare organizations to focus on staff well-being, open up lines of communication, and improve the workday experience. But the right technology—easy to use, mobile friendly, and able to take on the most monotonous administrative tasks—can make a huge difference, allowing staff to focus on more complex and rewarding work: caring for patients.
Learn how the Oracle ME platform can help your organization improve the employee experience.
What is the cost of employee turnover generally?
Employee turnover costs US companies an average of $50,000 per worker, not factoring in the heavy burden on the employees who stay.
How is the cost of employee turnover calculated?
To calculate turnover costs, dig into the numbers. Calculate the cost to hire contract fill-ins for the vacant position and the cost to recruit and hire the new employee (including job postings, managerial and HR time, and background screenings). Also factor in onboarding and training costs, as well as productivity costs as the new hire ramps up. The latter is usually calculated as the cost of a new hire’s salary and benefits during their first 30 to 90 days, when they’re doing more training than work.
What is the cost of nurse turnover?
The average cost of turnover for a staff registered nurse in the US is $46,100, with an average range of $33,900 to $58,300, according to the 2022 NSI National Health Care Retention and RN Staffing Report from Nursing Solutions Inc., a national nurse recruitment agency. The average time needed to replace a nurse is about 87 days. Nurses in some fields, including emergency services and behavioral health, are leaving at accelerating rates, with cumulative turnover rates that exceed 100%. (This happens when jobs need to be filled over and over—for example, an organization with 100 employees may have 50 positions that are filled by employees who stay long term and 50 positions where lots of turnover is the norm. Each terminated employee is part of the organization’s overall turnover rate.)
https://www.oracle.com/human-capital-management/cost-employee-turnover-healthcare

The Relationship Between Nurse Staffing, Quality, And Financial Performance In Hospitals
Little evidence exists on the relationship of nurse staffing and quality with financial performance in hospitals. This study aimed to measure the relationship between nurse staffing, quality of care, and
profitability in hospitals. This study used longitudinal panel datasets from 2006 to 2010, drawn from various datasets including the American Hospital Association Annual Survey Database, Medicare Cost Report, and Hospital Compare Data. This study used the random-effects linear regression model to measure the relationship between nurse staffing, quality, and profitability. In addition, we tested a mediating effect of quality on the relationship between nurse staffing and profitability. This study found nurse staffing’s significant association with quality and profitability in hospitals. First, compared to hospitals in the lowest quintile of RNs per 1,000 inpatient days, hospitals in the higher quintiles had lower pneumonia readmission rates, and higher total profit margins, operating margins, and cash flow margins. In addition, hospitals with lower pneumonia readmission rates were found to have higher total profit margins and cash flow margins. Lastly, the current study found that the positive relationship between RNs per 1,000 inpatient days and total profit margin and cash flow margin was partially mediated by pneumonia readmission rates. In conclusion, our finding that nurse staffing is positively associated with both quality of care and profitability in hospitals suggests that the idea of hospitals responding to financial pressures by cutting RN resources with a goal of greater profitability should be called into question. The influence of lower RN staffing levels on higher profitability for hospitals is uncertain, while it is possible that RN staff reductions may compromise the quality of patient care. Keywords: nurse staffing, registered nurse, quality of care, readmission rate, profitability, total profit margin, operating margin, cash flow margin, hospital.
On a practical level, the findings on the relationship between nurse staffing, and the quality and financial outcomes in hospitals can assist nurse managers and chief executive officers in identifying the optimal RN staffing level. These findings suggest that RN staffing level may be a strong predictor of quality and profitability and that the quality may mediate the relationship between RN staffing level and profitability in hospitals. This could be of particular interest to current hospital managers because of the payment reductions for excessive readmissions embedded in the ACA, which might have significantly affected the average profitability of some service lines in their hospitals. A lesson that can be learned from the past is that hospitals may attempt staff reductions in response to increased financial pressures as a result of payment reforms. However, as the findings in this research and the literature suggest, the reduction of nursing staffs may be related to an increase in adverse effect on the quality of patient care. The analysis results of this study demonstrated that a higher RN staffing level was associated with a lower pneumonia readmission rate, while the medium level of RN staffing level (≈ 7.7 RNs per inpatient day) had the highest profitability among general and acute care, non-federal government hospitals. Staffing decisions involve balancing between labor costs and the level of care required to fulfill healthcare needs of patients (Blegen, Vaughn, & Vojir, 2008). It is a matter of choice to hospital managers to decide what would be the most effective nurse staffing strategy for their hospitals in response to the HRRP.
https://journals.scholarpublishing.org/index.php/ABR/article/view/8745

The Effects of Nurse Staffing on Hospital Financial Performance: Competitive Versus Less Competitive Markets
Hospitals facing financial uncertainty have sought to reduce nurse staffing as a way to increase profitability. However, nurse staffing has been found to be important in terms of quality of patient care and nursing related outcomes. Nurse staffing can provide a competitive advantage to hospitals and as a result better financial performance, particularly in more competitive markets
In this study we build on the Resource-Based View of the Firm to determine the effect of nurse staffing on total profit margin in more competitive and less competitive hospital markets in Florida.
By combining a Florida statewide nursing survey with the American Hospital Association Annual Survey and the Area Resource File, three separate multivariate linear regression models were conducted to determine the effect of nurse staffing on financial performance while accounting for market competitiveness. The analysis was limited to acute care hospitals.
Nurse staffing levels had a positive association with financial performance (β=3.3; p=0.02) in competitive hospital markets, but no significant association was found in less competitive hospital markets.

Optimizing the Role of Nursing Staff to Enhance Physician Productivity: One Physician’s Journey
After completing my family medicine residency a few years ago, I immediately joined a private group practice with eight family physicians and two nurse practitioners and inherited a nearly full patient panel from a retiring family physician. I naively assumed that transitioning from residency to private practice would decrease my workload and increase my quality of life, but after a hectic first year, I knew that something had to change for my professional life to be sustainable. I was spending way too much time working and could see that the complexity of practicing medicine would continue to increase in the years ahead.
I began to look for ways to cope and came across an article in Family Practice Management by Peter Anderson, MD, and Marc D. Halley, MBA.1 The article described a new model in which a physician works simultaneously with two clinical assistants – a registered nurse (RN), a licensed practical nurse (LPN), or even a capable medical assistant (MA) – allowing them to assume more responsibility for each patient encounter so the physician can focus on the patient and medical decision-making. The additional nurse responsibilities include gathering an initial history (including the history of present illness, HPI; review of systems; past medical, social, and family history, PSFH; and health habits) and then staying in the exam room to document the physician encounter, order needed tests, print handouts, send prescriptions to the pharmacy, and complete the note including the assessment and plan. By shifting many of the ancillary physician tasks to well-trained clinical assistants, the physician can focus on what he or she is uniquely trained to do – provide high-quality acute, chronic, and preventive care in the context of a therapeutic relationship. After discussing this idea with my nurse (an LPN) and practice manager, we decided to try this new model.
My nurse and I started slowly, selecting several days where we would see fewer patients, thereby allowing additional time to learn our new process. It was a significant adjustment for both of us. She was now in charge of the documentation (and thus the computer), and it became necessary for me to clearly verbalize every aspect of the visit, including the physical exam, the assessment, and the plan for treatment or additional workup (labs, imaging, medications, referrals, etc.). We used Anderson and Halley’s model as our starting point, but soon our process evolved based on our own skills and strengths, the needs of our patients, and the limitations of our office space, schedule, and electronic health record (EHR). After experimenting for a month, we were both convinced that we were ready to fully commit to this new model and decided to hire a second nurse. Because we had spent significant time fine-tuning our system, the training process for our second nurse (also an LPN) was relatively smooth, and my original nurse was able to do the bulk of the teaching.
Every new process requires some experimentation and modification in the early stages, and for our practice key adjustments occurred in the following areas:
Communication with nurses. When we first began, I would handwrite my assessment and plan for each patient encounter to ensure accuracy. Quickly, my nurses let me know that this was a waste of time. Instead, they suggested that I clearly explain each diagnosis and associated plan to the patient, and they would capture the information as I spoke. The nurses have also demonstrated that they can capture patient instructions as we discuss them, and they now typically print those instructions at the conclusion of each visit. Today it is unusual for me to type or handwrite anything during an office visit.
Access to patient data. Each of our exam rooms has a desktop computer that we use to navigate the EHR. Lab and imaging results import electronically into the EHR, as do many of our consult notes. With my nurse in the room using the computer during the office visit, I lost the ability to peruse the chart during the visit, so I began to use an iPad with our wireless Internet connection to view a read-only version of the chart. The iPad also allows me to review the history related to each problem, the problem list, and current medications without pulling my nurse away from her documentation responsibilities.
Chart review. As we progressed with our new model, I continued to gradually shift more responsibility onto my nurses’ capable shoulders. They assumed responsibility for immunization status (checking status for adults and children, administering needed vaccines, creating catchup schedules, etc.), preventive care, and even some basic chronic disease management (confirming annual diabetic eye exams and referring as needed, ordering annual lipid panels when appropriate, etc.). The nurses found that in opening a visit note, they were essentially doing a thorough chart review including reviewing, updating, and sorting the problem list; reviewing preventive care needs; sorting the medication list; reviewing and reorganizing the PFSH and health habits; starting the HPI by searching the chart for any prior tests or visits related to the chief complaint (as recorded by the front desk staff when scheduling the visit); and even starting the assessment and plan portion of the note by listing the relevant diagnoses. It was not possible to accurately complete such a chart review between patients, so my nurses agreed to arrive about an hour before our first patient each day to allow additional time for this work.
Patient check-in form. We have continually worked to implement processes that improve patient flow and efficiency during office visits. One of our more successful processes involves using a patient check-in form. Early on, it became apparent that the rooming process was a bottleneck in our patient flow because of the need to confirm problems, medications, allergies, social history, family history, habits, etc. I had asked my nurses to attempt to quickly update these at each office visit, and it turned into a time-consuming process, particularly for complex patients on multiple medications. To expedite the process, we worked with our EHR support staff to create a one-page document that lists a patient’s medications, allergies, family history, social history, health habits/risk factors, pharmacy of choice, and advance directives. These forms are printed directly from the EHR during the morning chart review and are given to the front desk staff to pass out to patients when they arrive. This allows patients to review much of their history while sitting in the waiting room and allows the nurses to address only changes that need to be made. As an added benefit, patients appreciate that we put time into prepping for their arrival rather than handing them a blank form to complete.
Patient privacy. I was concerned that having a nurse present in the exam room might be a distraction for patients or make them uncomfortable sharing sensitive information. While we did receive several questions initially about the nurse being in the room, I have been pleasantly surprised by how many patients don’t even seem to notice. There are occasional instances when it is evident that a patient would be more comfortable without a nurse present during the visit, and the nurses can usually ascertain this while rooming the patient. Overall, feedback has been amazingly positive. Rather than viewing the nurses as an intrusion, patients appreciate the additional resources that my nurses have become. They also seem to recognize that the nurses’ presence allows me to be fully focused on them, rather than trying to manage charting, test orders, referrals, and refills while providing their care.
Space, workflow, and scheduling issues. Because my colleagues were not implementing the same practice model that I was, I was careful to limit the impact on them. To create a new workspace for my second nurse, I cleared some supplies from an unused desk, purchased a new computer, purchased a new office chair, and moved an unused phone. I typically have access to only two or three exam rooms while seeing patients (the Anderson and Halley model suggests three to five exam rooms), but I have not asked for more. I have found that even with two exam rooms I am considerably more efficient under this model.
While both of my nurses participate in patient visits throughout the day, they typically have short breaks between patients and can use this time to manage phone calls, medication refills, and other peripheral nursing issues. Because of this, we have not needed to schedule additional time for the nurses to manage these tasks, although we have utilized our group’s two full-time triage nurses for support on our most hectic days.
The transition to our new model has probably been most difficult for our office manager and our group’s lead nurse. A new process was required to schedule my nurses, and it can be tedious to manage schedules when I am out or one of my nurses is out. I have just recently started training some of our other office nurses in the new model, but previously I would have to resort to my old single-nurse system if one of my two nurses was out of the office.
Ongoing improvement. To fully implement this system requires nurses who are motivated and willing to assume more ownership over each patient encounter. The nurses’ knowledge of each patient and their overall medical knowledge has grown as a result of their active participation in each visit, and they have learned by watching how I make decisions and conduct the medical workup. I also continue to teach them in a more formal manner by using interesting cases that we see, and I have learned this model requires an ongoing commitment to training. I started out meeting with my nurses for one hour each week, and even though I have been using this system for almost two years, I continue to meet with them at least twice per month. During these meetings I elicit feedback about problems or inefficiencies, provide feedback on recent chart notes, and provide teaching about changing medical standards of care. My nurses are now often the ones to identify problems and suggest appropriate changes to improve our model and the care we provide. These routine meetings have created a culture of teamwork and a continual focus on innovation – traits that will likely serve us well in the ever-changing world of medicine.
Two years into the model, we can report positive results.
Patient care statistics. The organization I work for monitors patient care data, generating physician report cards for preventive care and chronic disease management. Since implementing this new practice model, I have seen an improvement in most of my report card measures, particularly those that rely more on my nurses to complete. For example, the table below shows improvements in virtually every category of diabetes care, with a particularly large jump in the percentage of diabetes patients who have received foot exams, a task I have completely turned over to my nurses.
Since implementing my new practice model, in which nurses take greater responsibility for certain aspects of the patient visit, I have seen improvements in most of my report card measures, including those for diabetes care, shown here.
| Percentage of diabetes patients | |||
|---|---|---|---|
| Diabetes measures | Goal | Old system | New system |
| A1C > 9% | < 15% | 5% | 0% |
| A1C < 7% | > 40% | 53% | 64% |
| Blood pressure > 140/90 mm Hg | < 35% | 22% | 7% |
| Blood pressure < 130/80 mm Hg | > 25% | 53% | 64% |
| Eye examination completed | > 60% | 47% | 48% |
| Smoking status and cessation advice or treatment provided | > 80% | 98% | 98% |
| LDL > than 130 mg/dl | < 37% | 15% | 9% |
| LDL < 100 mg/dl | > 36% | 58% | 62% |
| Nephropathy assessment completed | > 80% | 95% | 95% |
| Foot examination completed | > 80% | 60% | 79% |
Finances and productivity. The costs incurred with this new model can be divided into two categories: initial startup costs and ongoing costs. I estimate that my initial startup costs were in the range of $15,000. This includes the fairly nominal cost of additional office equipment (computer, office chair, etc.) and the more significant cost of slowing down my days as I brought both nurses up to speed on the new system. The only significant ongoing cost is paying the salary and benefits of my second LPN, approximately $8,000 per quarter. This is less than you might expect because four months after transitioning to this new model, I made a personal decision to decrease my full-time equivalent (FTE) status from 1.0 to 0.75. Thus, I am not responsible for the full salary of my second nurse. The remainder of her time is allocated to other parts of the practice.
My FTE change makes it nearly impossible to calculate how my practice change has affected revenue, but I can say that my office productivity has increased. We measure productivity in terms of patient visits per half-day and average charge per patient visit, which we track based on work relative value units (RVUs). Since moving to this new system, I have seen my patient visits per half-day increase by 15 percent and my average charge (work RVU) per office visit increase by 10 percent (see the graph below). Because some of our practice costs are divided based on productivity, this increase in my productivity has led to a relatively minor, but ongoing, increase in those costs.
Under my new practice model, patient visits per half-day have increased 15 percent and work relative value units (RVUs) have increased 10 percent. These numbers reflect an eight-month average before and after changing to the new model.
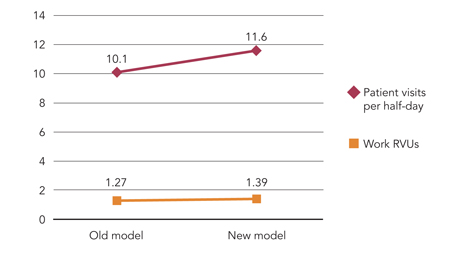
Although this new model has certainly brought an increase in expenses, I have seen a much greater increase in productivity and revenue, which has allowed me to maintain an annual income above the national median of $160,000 for a full-time family physician, despite having decreased my FTE status to 0.75.
Nurse and patient satisfaction. During this transition I have regularly asked my nurses for feedback regarding their satisfaction with our change, and when there have been frustrations or difficulties, I have done my best to work creatively with them to correct those. At this point, I am happy to report that my nurses are both very pleased with our current system. My original nurse reports that “Overall, I am very happy with the two nurse system. My favorite thing about it would be that I get to see from start to finish the entire diagnostic and treatment process. It allows me to become educated on each patient’s history and treatment plan, which in turn allows me to provide appropriate care and to be a better advocate for that patient. While working so closely together, I’ve been able to gain an understanding of how Dr. Anderson practices, and I have become more confident in myself and my own skills. Our care as a team has become significantly more thorough, and we are able to focus now on providing comprehensive care to each individual.”
Although we have not conducted a formal patient survey, the feedback we have received from patients has been almost universally positive. Patients are happy to have my undivided attention while in the exam room, they appreciate getting so much done with each office visit, and they are grateful that my increased efficiency has allowed me to be more available for same-day appointments.
This journey in restructuring my practice model has led me to a place where I am able to focus more on my patients, provide higher quality care, be more productive, and have happier employees. As physicians, we should not view ourselves as beholden to old models of care. Instead, we ought to view ourselves as empowered to institute fundamental changes to our work. The practice of family medicine is likely to get more demanding in the years ahead, and it is our opportunity and responsibility to build innovative practices that meet these demands while enabling excellent patient care, employee satisfaction, and a sustainable and meaningful personal life.

10 Best Practices for Increasing Hospital Profitability
Industry experts say that hospitals wishing to increase their profitability can focus on two key areas — reducing costs and increasing reimbursement. Here are 10 best practices for increasing hospital profitability by reducing costs and increasing revenue and reimbursement.
Because labor is the largest single expense for hospitals, it is critical that hospitals are not over- or under- staffing their facilities.
Hospitals leaders can cosider the use of flexible staffing, such as part-time or hourly employees, and adjust staffing based on patient census data. Leaders should also monitor the efficiency of this staffing by continuously reviewing benchmarking data such as hours worked per case.
Amy Floria, CFO of Goshen (Ind.) Health System, says that her facility monitors patient volume on a daily basis and adjusts staffing accordingly. “We adjust our nursing staffing every eight hours after looking at our inpatient volume and expected discharges and admits,” she says.
Kevin Burchill, a director at Beacon Partners, a healthcare management consulting firm, agrees that staffing must be adjusted daily. “The easiest thing that a hospital can do to improve profitability is for the senior management team to assume responsibility for the day-to-day performance of an organization and look at the organization’s performance in real time,” he says. “You must shift to an emphasis on the day-to-day, not pay-period to pay-period or month-to-month.”
It is important that concerns regarding efficient staffing are communicated throughout the organization and that hospital leaders work in collaboration with physicians. Donna Worsham, COO of National Surgical Hospitals, suggests that hospital leaders share staffing efficiency benchmarking data with unit managers and provide feedback regarding the productivity of the unit.
Flexible staffing is especially useful for OR nursing staff. OR managers should review clock-in times versus surgery-start times and determine if their staff is consistently arriving before a surgery actually begins. If this is the case, mangers can utilize flexible staffing to allow nursing staff to arrive later so that when surgeries run over, no overtime expenses are incurred, says Ms. Worsham.
Other facilities are saving in staffing costs by reducing benefits for full-time staff. Goshen Health System, for example, deferred merit increases, reduced paid vacation time and suspended its retirement matching program in response to the current economy, according to Goshen’s CEO, Jim Dague. Goshen reduced employee dissatisfaction in response to these cuts by soliciting employee feedback on which benefits to reduce, thereby building organizational support for the changes. In addition, Goshen’s executives took a voluntary 20 percent cut in order to help sustain the system through the recession.
Joe Freudenberger, CEO of OakBend Regional Medical Center in Richmond, Texas, agrees that staff must buy in to any reductions in hours and shifts worked that will personally affect them in order for the hospital to remain successful. He says that hospital leaders must communicate the reasoning for these changes to the staff before making them. “If we call off staff, they see it as personally hurting their income when we need to help them understand that it is actually preserving their income by maintaining the financial viability of the hospital,” he says. “It may be obvious to us that we’re calling them off because we have a significant reduction in patient volume, but we need to communicate that to them for them to understand the financial realties we face.”
Although some staffing cuts may be necessary, hospitals should be careful not to take a blanket approach to layoffs or cuts in services. Hospital leaders must take a close look at their business before making cuts.
“Don’t make the same mistake everyone else does — don’t look at bottom line, determine that you need to cut $1 million, for example, and then cut 10 percent across the board. Doing so will trim some fat but will cut meat and bone in other areas,” says Mr. Burchill.
He suggests that hospitals assess each program individually and determine which ones are what are winners and losers. “You do not want to cut areas that you should be doing more of or that are already profitable,” says Mr. Burchill.
Hospital leaders can reduce supply costs by working with vendors to improve contracts and encouraging physicians to make fiscally responsible supply decisions.
“When it comes to supply costs, you must drive this expense or the vendor will drive it for you,” says Ms. Worsham.
Hospital leaders should not shy away from approaching vendors for discounts. Goshen’s IT director recently requested a discount on the health system’s contract for IT maintenance due to current economic conditions and successfully received a discount that saved the hospital 15 percent on this contract, according to Ms. Floria.
Hospitals can also reduce supply costs be reducing the number of vendors. Goshen, for example, is in the process of reducing the number of vendors in its surgical suite and aims to eventually scale the vendors down to 4-6 companies. “This action is expected to save us at least a million dollars in supply costs,” says Mr. Dague.
Another way in which hospitals may reduce supply costs is by requiring vendors to submit purchase orders for any equipment or implants that are not included in a negotiated, written agreement with the facility. “All of our vendors sign agreements that any purchase orders must be submitted at least 24 hours before a procedure and must be approved by the materials manager or the CEO, or it’s free,” says Ms. Worsham. “If you don’t require this, vendors will drop off the invoice for a pricey piece of equipment or implant after the procedure has already taken place and walk out the back door, which can greatly hurt your profitability.”
All hospitals can benefit from tightening up the efficiency of their operating rooms, but it is especially critical that less busy facilities ensure that their ORs are used as efficiently as possible.
“Hospitals need to review block time utilization,” says Ms. Worsham. “Physicians who are assigned more time than they are using are hurting your profitability.”
Ms. Worsham suggests that hospital OR managers work directly with physicians to make OR utilization more efficient.
“When physicians’ schedules create gaps in the OR schedule, it effects a hospital’s ability to staff effectively, which can create significant labor costs for the hospital,” says Ms. Worsham.
Hospitals should work to encourage physicians to become more concerned about the costs of supplies and other activities, such as unnecessary tests and inefficient coding processes that may drive up hospital costs.
“Hospitals today have a unique opportunity to leverage physicians’ interest in having hospitals help to stabilize their incomes with the hospitals’ needs to involve physicians in cutting costs and improving quality,” says Nathan Kaufman, managing director of Kaufman Strategic Advisors, a hospital consulting firm.
Hospitals can encourage the use of products from vendors that are cost-effective, but still high quality, especially in areas such as orthopedic implants, which can be considerably costly for hospitals. In addition, experts say the use of protocol-based care can reduce costs associated with unnecessary tests or treatments.
Mr. Freudenberger says that one of the biggest mistakes hospitals make is not engaging medical staff in profitability. “Physicians have a huge role in maintaining hospital profitability, but unless you give them a reason to be concerned with a hospital’s profitability, they will make choices in what and to whom they refer services that will not consider the implications to the hospital,” says Mr. Freudenberger. “Hospital leaders should work to help medical staff understand the connection of their referrals to the hospital’s viability so that their referral decisions reflect the value they place on the hospital.”
During tough economic times, some hospitals may benefit from outsourcing or partnering with other organizations for certain services, such as food and laundry services, and even, in some cases, clinical services.
“Some hospitals see these economic times as an opportunity to outsource unprofitable services,” says Mr. Burchill.
By outsourcing certain services to more efficient providers, hospitals can share the savings with the service provider. However, hospitals must be sure to select truly efficient providers.
“Outsourcing is clearly a smart thing to do if an organization can gain greater efficiency through finding a larger-scale operation; however the provider must be more efficient than the hospital,” says Kevin Haeberle, executive vice president, HR capital, for Integrated Healthcare Strategies.
Oftentimes, hospitals outsource services such as laundry, food and nutrition, information technology or human resources because they do not have the capital to invest in the equipment upgrades or training that is needed to increase the efficiency of their internal service. In these cases, the decision to outsource may not directly be related to profitability but instead the “lacking of funds for the investment required to make current services viable,” says Mr. Haeberle. However, this decision can improve profitability in the long-run by allowing hospitals to use funds for more profitable services.
Some hospitals have also begun to outsource clinical services such as emergency room staffing and anesthesiology in an attempt to become more efficient. Because these staffing groups employ a large number of specialty physicians, they may be able to provide more efficient services, especially in clinical areas that require around-the-clock coverage where the demand for services is high.
Mike Mikhail, MD, vice president of client services for Emergency Physicians Medical Group, says that hiring an emergency department management company can help to improve the profitability of hospitals whose demand for emergency services exceeds its emergency treatment capabilities. “An emergency management group can help make the emergency department more efficient by introducing management oversight and best practices, allowing more patients to be seen and keeping others from leaving to find another hospital,” he says. “Because a majority of hospital admits come from emergency walk-ins, driving more patients through an ER will create more admits, and therefore more profit for the hospital.”
An increasing number of hospitals are joint venturing with local physicians and surgery center management companies to offer outpatient services through the development of a surgery center.
According to Clete Walker, vice president of development for Surgical Care Affiliates, hospitals are beginning to focus on the need for a comprehensive outpatient strategy and recognizing the need to partner with doctors to effectively execute on this strategy. Mr. Walker reports that he has seen an increased interest from hospitals in joint venture arrangements for outpatient services.
“More and more hospitals are realizing that their core competency is providing inpatient care; their outpatient cases are more costly per case and take up more of the physician’s and patient’s time than they do at an ASC,” he says. “As a result, hospitals are competing with physicians for outpatient cases. Hospitals with joint-venture agreements, however, do not have to compete with the physicians.”
Hospitals can leverage their standing in the community to partner with local physicians to share the revenue generated by efficient outpatient cases.
“We are in lean times, and lean times call for us to rethink our strategies,” says Mr. Walker. “It’s better for physicians, hospitals and other groups to work together to provide an efficient delivery system for patient care than for the groups to compete.”
Identifying and attracting additional physicians to bring cases to your hospital is another way that hospital leaders can increase profits. Physician-owned hospitals can bring in additional physicians as partners, while other types of facilities can recruit new physicians who are willing to perform cases at their hospitals.
“New physicians will bring in more cases and grow your profits,” says Ms. Worsham.
Ms. Worsham suggests polling your medical staff for names of local physicians to target and inviting them into the facility. During the visit, Ms. Worsham recommends that hospitals work to “wow” the target physician. “We work tirelessly to promote the services we can offer them,” she says.
When a new physician begins performing cases at one of Ms. Worsham’s facilities, that physician is assigned a concierge. “We have strong internal programs in place for this first day. A concierge is assigned to each new physician who provides them with a tour facility and walks them through every aspect of their day,” says Ms. Worsham.
Hospitals may also be able to grow case volume and profits by adding new service lines. However, hospitals need to be careful to do their homework on the expected profitability and ROI for any new lines added, especially in a market where access to the funds required to invest in new service lines may be tight.
“You have to look at what the market needs are and where you’re going to get the referrals from,” says Ms. Worsham. “Meet with local physicians and interview them about their needs and the number of cases they see that could utilize a new service.”
Hospitals should also be sure to examine the competitive landscape for any new service line.
Ms. Worsham reports that her facilities have had great success from adding a hyperbaric service line because few competitor hospitals were offering this service.
Hospitals that use hospitalists to care for patients can benefit from the more efficient care and better documentation that specialized hospitalists can potentially provide.
“A protocol-based hospitalist program can increase efficiency and help to reduce the length of stay for patients, which can increase case volume without the need for additional beds,” says Mr. Kaufman.
Hospitals should consider employing these specialists as a means to improving care and enhancing their bottom lines, according to Mr. Kaufman.
Stephen Houff, MD, president and CEO of Hospitalists Management Group, says that hospitalist groups can provide effective care to patients and possibly increase reimbursement. “Hospitalists may be the most reliable and cost-effective means available for hospital leaders to transform medical delivery in their health system,” he says. “Through shared vision, an effective hospitalist team partners with hospital leadership to improve patient safety and access, streamline care, improve patient and family satisfaction, enhance reimbursement via improved clinical documentation and provide seamless transition to post-discharge care.”
One of the most important ways that hospitals can improve their profitability is by continually evaluating and renegotiating their managed care contracts.
“Hospitals must demand their fair share of premiums from third-party payors in order to subsidize the underpayment of Medicare and Medicaid,” says Mr. Kaufman. “Hospitals need to focus on reducing their cost structure as much as possible to approach breaking even with Medicare reimbursement rates, but that only goes so far.”
Mr. Kaufman recommends that hospitals only agree to contracts that reimburse at 130-140 percent of cost. “If a facility is not big enough or strong enough to get these rates, then they should look at merging with a larger facility,” says Mr. Kaufman.
Ms. Worsham suggests that hospitals perform a profitability analysis by payor and by procedure in order to determine where a facility is losing money and identify any trends. She also suggests that hospitals evaluate older contracts due to changes in severity-based DRGs and carve out the reimbursement of implants in order to ensure they are reimbursed appropriately for the costs associated with these.
Ms. Worsham also suggests that hospitals evaluate contracts on a quarterly basis, even if the contract is not near expiring. She suggests that hospital leaders examine the contracts with the following questions in mind:
• Is revenue where we thought it would be given reimbursement rates and volume of policy holders?
• Are we being paid as agreed upon in the contract?
• Are we being paid in a timely manner?
Contracts that are determined to be “high risk” should be renegotiated. Make sure your contracts contains a material harm clause, which will allow you to readdress terms of contracts that have become financially harmful to the facility, according to Ms. Worsham. Renegotiating contracts can be very valuable — one hospital Ms. Worsham advises will gain $500,000 this year due to renegotiations.
Hospitals that focus on enacting these best practices are likely to see improvements in their profitability; however, hospitals can also benefit by using today’s economic conditions as an opportunity to improve their overarching approach to business, creating a more sustainable organization in the future.
“When profits were high, hospitals had the luxury of being sloppy in some areas; now we must run a tighter ship,” says Ms. Floria. “This will benefit the industry in the long-run.”
Hospitals can also use this opportunity to find creative solutions to problems that plague their facilities.
Goshen Health System, for example, recently enacted a program in which the hospital pays the premium required to sustain Cobra benefits for recently laid-off patients seeking care. “We are willing to be creative with our patients,” says Ms. Floria. “We pay for benefits when certain patients cannot. The revenue we receive from caring for these patients recoups this cost and provides us with additional cash flows that likely would have been uncollected or written off to charity care or bad debt.”
This idea, which was enacted during lean times to improve profitability, will continue to benefit the hospital’s bottom line, even when profitable times return.
Contact Lindsey Dunn at lindsey@beckersasc.com.